
There’s been some discussion about scientists being attacked for telling the truth. I do, of course, think that this is a real issue, but I also find myself somewhat frustrated by all of this. It’s hardly surprising to anyone who is aware of what has happened in the climate context.
Given that epidemiologists must have been aware that their research could end up being associated with decisions that some will find objectionable, why weren’t they somewhat more prepared for this? It’s clearly impossible to competely avoid these kind of attacks, but it doesn’t feel like much thought has gone into this at all. For example, it would probably have been much more difficult to attack the scientists if the advice appeared to be the consensus view of the relevant scientific community, rather than appearing to come from one research group (and, to be clear, I’m using the term appearing here intentionally).
I also find myself now to be somewhat more in agreement with those who object to the term listen to the science. I’ve never had much of an issue with it, since it is clearly a simpistic narrative intended to mean something like listen to the scientists and do something to address the risks that they’re highlighting. However, it’s clear that science doesn’t tell us what to do, and the responsibility for making decisions lies with policy makers, not with scientists.
The problem with promoting the idea that policy makers must simply listen to the science, is that they can point fingers at the scientists if their decisions are unpopular, or ineffective; “we just listened to the science”. So, you have to be careful that these simplistic narratives don’t end up being used against scientists by people who disagree with the decisions that were made, or who are trying to deflect the criticism from themselves back onto the scientific advisers.
To be clear, I do think we should defend scientists against unfair attacks by the media and we should continue to stress that scientists are simply advisers; the responsibility for making decisions lies with policy makers, not scientists. However, I also think it’s important that scientists who do engage publicly, especially with policy makers, are aware of the environment in which they were operating, and try to learn from other similar situations.

I think you raise a very important point. However, you refer to a consensus. Consensus is not what science is about. It is about evidence. There is obviously a difference of view both in climate science and now in the case of the epidemiology. Models are not evidence. They are only as good as the assumptions and the data. Two models might agree, but they could both be wrong. In the case of climate science, we see scientists at their worst with the IPCC mob, and that is what they are, slinging insults at those who disagree. Science is about cooperation and discussion when there is a difference of view in order to arrive at the “best” science as we know it. This does not happen today because money and politics, not the search for truth has taken over science.
Evidence must be the basis of the final agreement. In the case of climate science which is now essentially about human caused global warming, there must be evidence, through observation of the actual climate that human released CO2 can be directly linked to temperature change. Nobody has yet proposed how those observations can be made. We cannot create a physical model of the atmosphere and models are just models, not evidence. In the case of the climate the timescale for change in long even though many activists say otherwise.
But with the virus, immediate action was needed, at least according to almost every government. The UK scientist has a reputation for inaccurate predictions and yet he was used together with his usual extreme predictions and hence fear and panic was generated.
In the end it is the politicians who decide policy and they must be accountable for the chaos they have created. We know that will not happen. At best they will be kicked out and and retire on a fat pension.
If Small Hands was not playing with himself 247 he still would not have listened to the scientists. But don’t panic, Small Hands said it will just go away. Seriously said so! Small Hands has been silencing the CDC and scientists because he does not want to scare people. You know, Small Hands has an erection coming up so must make the economy go ZOOM!!!
Meanwhile NYC workers are dying trying to keep the subway cars clean. Seriously dying!
Obama said we are not a nation of laws anymore or maybe it was the rule of law is falling apart or some such. Seriously said so!
I dined out last night and none of the patrons were wearing masks but all of the waiters and cooks were wearing masks. The restaurant was more concerned about the patrons getting infected then they were for their own workers health.
OK, so I made that one up. Me dining out, that is. The rest is much closer to the truth though.
Obama actual partial quote ” … but our basic understanding of the rule of law is at risk.”
Morpheus Kuhn wrote about scientific paradigms and their overturning. A consensus is an expression of a paradigm – a set of beliefs that scientists generally hold to be true (provisionally). Science does involve consensus, you don’t even have to be a Khunian to accept that. For example I suspect there is a pretty good consensus among astronomers about stellar evolution, amongst biologists about DNA, among climatologists about the greenhouse effect. You may not like that, but it is true.
As to what causes there to be a consensus on a paradigm? Evidence!
As long as we are going there again
http://rabett.blogspot.com/2015/12/normal-science.html
The existence of a scientific consensus in a field implies a knowable nature.
Because a problem has not yet been solved within the current consensus does not mean that a completely new consensus is needed. Experience shows that it is more likely the observation or theoretical work has overlooked some factor or made a mistake. It is only when a large body of work cannot be understood within the current consensus that scientists start looking for a new paradigm. Major changes in the consensus, Kuhn’s paradigm, are almost without exception extensions of previous paradigms rather than refutations. The new paradigm extends the region of validity of the old.
To this Eli can add a bit describing a useful scientific paradigm. It is characterized by coherence, consilience and consensus, the rule of the three Cs.
Coherent paradigms are consistent
Consilient, paradigms explain much efficiently and are coherent
And consensus means just what Kuhn said, that members of the community can talk with each other in the framework of a coherent and consilient paradigm
Eli,
Thanks.
Morpheus,
As Eli points out, science often (mostly) does involve being aware of a consensus. Scientists don’t reinvent the wheel everytime they do some research; they’re often working within some framework that is currently supported by the evidence. This is what I would regard as a consensus position. Of course, some scientists might be trying to challenge this, but even doing so requires an understanding of what it is.
Also, the point I was making is that what policy makers probably want to know is some kind of consensus position that most in a research field would agree with. This doesn’t mean that there’s certainty about this (i.e., the consensus position can still include uncertainties) but it would preferable to only getting the views of a minority.
Meanwhile those Swedes, what a smart bunch, they went the herd immunity route, thinking that their own economy would not collapse. Then someone else, much smarter then those Swedes, said, well we do have imports and exports, So that their economy will still collapse regardless. because it is still in large part interdependent with the rest of the World’s economies, which are now in a global dumpster fire. Anyways, they sort of disappeared that someone else, but before that happened, that someone else left this …
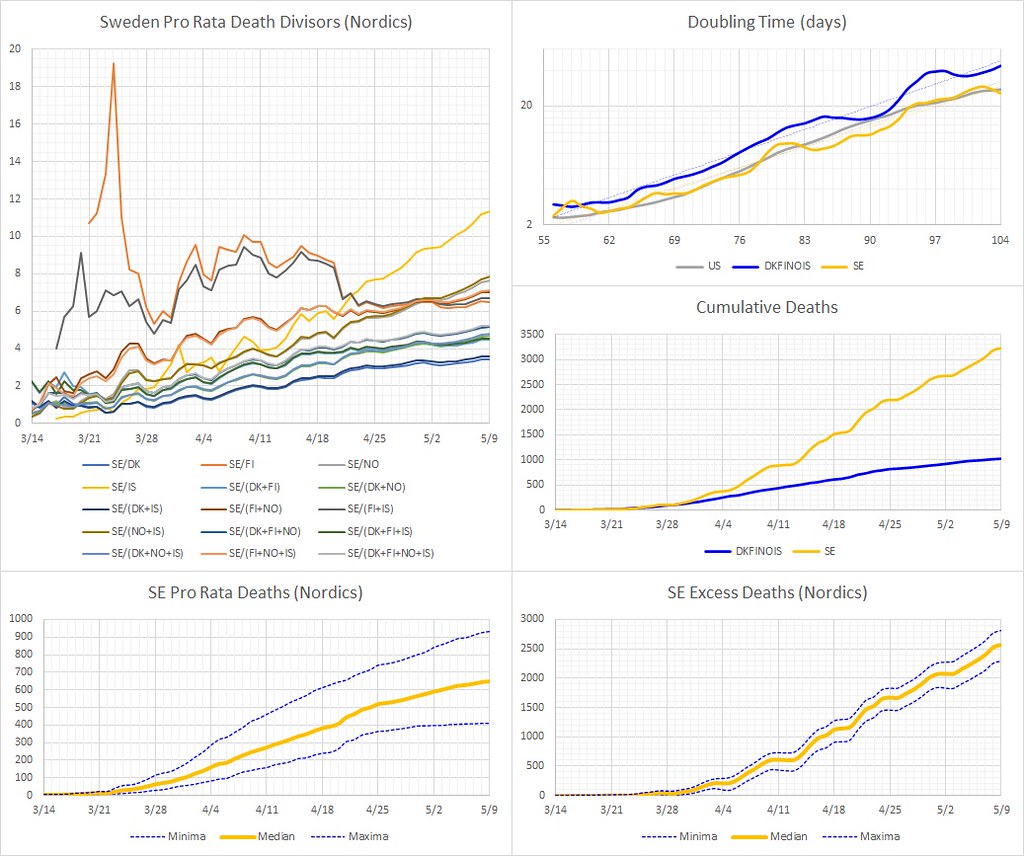
Same drill as the last time, outliers dropped (IS, IS+FI and FI, although the two FI combinations look OK over these past two weeks, suggesting that any initial lags are now small relative to eight full weeks of data). SE now has ~2600 excess (median) deaths compared to its Nordic neighbors (regardless of the remaining 12 combinations, pro rata ~ per capita basis).
Describe what a scientific publication would look like if science had no consensus. Lol.
Anders –
> For example, it would probably have been much more difficult to attack the scientists if the advice appeared to be the consensus view of the relevant scientific community, rather than appearing to come from one research group (and, to be clear, I’m using the term appearing here intentionally).
I think you underestimate the abilities (or perhaps level of motivated reasoning) of those who seek to undermine the work of scientists that produce work they don’t like. For example, the existence of a consensus in climate science, it doesn’t seem to me, makes it even remotely difficult for “skeptics” to attack climate scientists.
> Evidence must be the basis of the final agreement.
Agreement… like in consensus, Allan?
Everett –
> Then someone else, much smarter then those Swedes, said, well we do have imports and exports, So that their economy will still collapse regardless.
https://www.cnbc.com/2020/04/30/coronavirus-sweden-economy-to-contract-as-severely-as-the-rest-of-europe.html
That said, I’ve read that Swedes in government are blaming the economies in other countries for Sweden’s economic problems during COVID-19. That seems rather like bullshit CYA to me. The likelihood of an economy avoiding a dramatic downturn with many citizens getting sick and dying, and many citizens fearing getting sick and dying, seems rather small to me irrespective of the effect that downturns in other countries’ economies might have.
“To be clear, I do think we should defend scientists against unfair attacks by the media ”
We ought to defend politicians against unfair attacks by the media as well. IMHO the overly adversarial manner of the media is partly responsible for the way politics is the way it is. We, the consumers are partly responsible for the way the media is – if we didn’t want showy confrontation rather than rational analysis, the media wouldn’t give it to us. “panem et circenses”, except without the panem.
> The UK scientist has a reputation for inaccurate predictions and yet he was used together with his usual extreme predictions and hence fear and panic was generated.
You know, maybe it’s just me, or maybe y’all in the UK have a stiffer upper lip than us Yanks, but it seems to me that thousands of people getting sick and dying, and news of hospitals being overrun in China and Italy, might have just had a tiny impact of getting a few folks upset even without the UK scientist’s “extreme predictions..”
–snip–
…data shows that residents there were staying home well before their governors issued stay-at-home orders.
[…]
Almost uniformly across these states, people started staying home beginning on March 14.
https://fivethirtyeight.com/features/americans-didnt-wait-for-their-governors-to-tell-them-to-stay-home-because-of-covid-19/
–snip–
And BTW, with respect to this:
> The UK scientist has a reputation for inaccurate predictions and yet he was used together with his usual extreme predictions and hence fear and panic was generated.
In case anyone hasn’t gotten enough of this shit from the climate blogosphere – the parallels w/r/t epidemiological modeling are really quite remarkable even if they aren’t at all surprising. Check it out if you have the stomach:
https://statmodeling.stat.columbia.edu/2020/05/08/so-the-real-scandal-is-why-did-anyone-ever-listen-to-this-guy/
You would need to wade through the comments to see how full of crap the attacks against Furguson really are. dhogaza did yeoman”s work in breaking down the attacks on Furguson’s programming.
“Also, the point I was making is that what policy makers probably want to know is some kind of consensus position that most in a research field would agree with. ”
Indeed, even if consensus wasn’t an part of science, that doesn’t mean it isn’t part of how society uses science to inform policy.
Reminded of the Delingpole and Paul Nurse discussion about there being a consensual position on the treatment of someone”s cancer and that we would naturally follow it – from about 1:13
morpheusonacid:
If you quit taking acid, you might become scientifically meta-literate enough not to call the IPCC a mob. The AR5 Working Group I report, on the Physical Science Basis of AGW, does in fact represent a conservative consensus of publishing climate specialists at the time. At least, the US National Academy of Sciences says so:
Scientifically meta-literate non-experts acknowledge that if it’s good enough for the NAS, it’s good enough for them. At least, no one who isn’t a climate specialist knows enough to contradict them. If you think you do, it’s the acid talking.
Well, We have no idea if Ferguson was telling the truth but I’m willing to give him the benefit of the doubt. The problem here is that his science was wrong and his track record seems to be to mostly err on the alarmist side.
There are by now at least a score of serologic studies around the globe showing that COVID19 has already infected vastly more people than the spurious “case” statistics we all see trumpeted daily. These top line statistics are complete scientific rubbish. This means the virus is much less deadly than Ferguson estimated admittedly based on incomplete data. The best serologic study was probably in Miami Dade county where they did a random sample. Taking the fatality number for 21 days after the median testing date, the IFR is 0.17% to 0.31%. This is likely an overestimation as most people use a 14 day delay. This is 3-5 times lower than Ferguson’s initial estimates. That’s a very big difference. Extrapolating to the US population one then gets 6% to 11% excess mortality on an annual basis (everyone agrees that perhaps 2/3 of the fatalities would have died within a year from their underlying comorbiditis). Perhaps comparable to the Hong Kong flu in 1969. And probably comparable to the flu in the absence of a vaccine.
Further, as has been known from the beginning, this virus is vastly more serious for those over 65 or those who are already seriously ill. Even using Ferguson’s too pessimistic IFR’s those under 40 have a very low risk of getting seriously ill. Ioannidis and colleagues argue based on Italian data that for those under 65 who are healthy, the chances of death are infinitesimally small. This would have offered obvious opportunities for targeted strategies. In the US between 40% and 60% of fatalities have been among long term care facility residents.
The simple fact of the matter is that governments have made decisions based on extremely uncertain science whose estimates have proved to be quite wrong. Every competent epidemiologist knows full well that historically, estimates of IFR have declined, often precipitously. One would think that competent scientists would be aware of this fact.
I see that Schmidt, someone with no knowledge of epidemiology, attacks an expert with a very strong track record. Sounds like Gavin may be becoming a merchant of doubt. I was hoping for something more substantive.
Try this, David:
https://statmodeling.stat.columbia.edu/2020/04/19/fatal-flaws-in-stanford-study-of-coronavirus-prevalence/
I don’t think you have any experience in epidemiology either.
Well, You are quoting Gelman out of context. In the conclusion of that blog post, he says he has no idea if the result is right or not, and that Ioaniddis and coauthors are the experts. He is just complaining about lack of adequate supplementary data about the testing method.
But this is just normal science. Picking out one example of a controversy about one of a prominent scientists papers is meaningless. There are now at least 10 serologic studies around the world that confirm the Santa Clara studies main conclusions, namely, that “case” statistics underestimate infections by at least a factor of 10 and probably much more.
The fact that Ioannidis’ early scientific instincts have been borne out by later research merely makes me more likely to believe him. He’s being unjustly slandered on twitter.
dpy6629:
“I see that Schmidt, someone with no knowledge of epidemiology, attacks an expert with a very strong track record.”
I’m especially thankful that Ioanndis’s prediction in late March that without government intervention, he thought that about 10,000 would die in the US. Total. He went on to say that if the press weren’t publicizing it, that we’d never notice, because far more die of the seasonal flu every year.
10,000 without intervention. Here we are at about 80,000 and still going strong. We should be at 100K dead by the end of the month.
That is a strong track record, but maybe not in the direction you assume.
David –
Respect uncertainty. Wait until you have good evidence to draw conclusions. For examlle, if you want to assess an IFR based in serological studies you should be using random and representative samples. We don’t have that yet. Meanwhile, we have stuff like this:
https://www.healthleadersmedia.com/covid-19/study-puts-us-covid-19-infection-fatality-rate-13
And this:
https://www.google.com/amp/s/medicalxpress.com/news/2020-05-team-covid-infection-fatality.amp
Both of which put the symptomatic infection rate at 1.3%. There’s some evidence that puts asymptomatic infections at around 50%. Other evidence more like 20% (like the Diamond Princess – which given the conditions much have had a relatively high infection rate).
You do the math.
At any rate, we don’t have enough data to say. What’s funny about Ioannidis is that after saying the data is insufficient, he went on to say that the IFR is about the same as the seasonal flu. Of course that was after he extrapolated a rare from a non-random and non-representative sample. It’s quite remarkable how you insist that it’s just peachy keen to extrapolate a broadly applied IFR from non-representative sampling.
Quite remarkable.
Anyway David. Respect uncertainty. Wait for the evidence to catch up with your desire to advocate based on your political orientation.
Respect uncertainty.
Joshua:
Thanks for the shout-out, especially since the self-proclaimed experts in readability and quality of code saying that the IC model was shit decided to disappear after three or four of us showed how wrong they were.
And I hadn’t even gotten to the point of discovering that their claim that the model is nondeterministic when running in multi-processor mode is false.
Turns out that’s only true for generating the network (who belong to what house, etc), which is highly parallelized for speed. The distribution of the allocation of individuals is constrained. And once a network is generated (which takes significant CPU time), you can save it and run the model against it. These model runs are deterministic.
Just another example of how much you must dig in and understand code to refute shouting claims like “it’s not deterministic, so you can’t test it by running regression tests in multi-processing mode!”, made by people who don’t know WTF they’re talking about.
Joshua
“Respect uncertainty.”
And respect the dead …
My bad – the German study puts the it at .37%.
But we know that the rate in the US is quite likely higher than in Germany for a number of reasons. That German study did put the asymptomatic rate at around 20%
This was the other source that pegged the symptomatic rate at 1.3%:
https://www.managedhealthcareexecutive.com/news/uw-researcher-covid-19s-infection-fatality-rate-10-times-larger-flus
At any rate – the point being to respect the uncertainty, until we have better data.
David –
And BTW, also from that German study:
> For studies planned to take place across Germany with an estimated infection rate of approximately one to two percent a one percent false positive rate pose rather a problem.
So they estimated an infection rate in a more representative sample to be one to two percent.
I try to tell you to look at representativeness of the sampling but you just won’t listen.
Oh. One more thing, David.
> Miami-Dade researchers partnered with Florida Power & Light to randomly generate phone numbers and invite people to come to 10 drive-thru testing locations.
That’s not random sampling. It’s quite likely to have a self-selection bias.
Additionally, Miami-Dade is a hotspot.
You really need to think about sampling methodology some more. Oh, and respect uncertainty.
Joshua, I urge always writing the integer to the left of the decimal point even if that integer is zero. For example, 0.37%. This eliminates any possible confusion about the role of the dot.
Joshua, We’ve been over and over this many times and you have said all this many times before.
There are uncertainties here. That’s why all the good studies give a range of IFR’s. My main point is just that as evidence is accumulating, the best evidence seems to show IFR’s between 0.12% and 0.4%.
There is also the issue that the number of studies now is large enough that’s it’s unlikely all them are biased in the same direction. The number already infected is 10-80 times greater than the “case” statistics that are quite meaningless.
A lot depends on the age structure of a population. Ioannidis does recommend and I agree that we should protect the vulnerable. But for those who are under 65 and healthy, there is little objective danger of becoming seriously ill. That is shown by all the data, especially in the US and Italy (which Ioannidis and several Italian scientists analyzed), and even Ferguson’s estimates agree. I don’t think he breaks it down by pre-existing conditions, only by age cohort.
You’ve thrown up again a host of vague objections that don’t offer a meaningful challenge to the science.
From the Ioannidis first draft:
“…correspond to an infection fatality rate of 0.17% in Santa Clara County…[it may] be substantially higher in places where the hospitals are overwhelmed (e.g. New York City or Bergamo)…” plus the usual age-weighted stuff.
So far 0.15 % of Lombardy is listed dead of Covid and total mortality spiked more. 0.24 % of NYC is “confirmed” or “probable” covid deaths.
Nic Lewis ran Diamond Princess numbers on March 25th:
“Accordingly, the [Imperial study source] central estimate for the Diamond Princess death toll, of 12.5 eventual deaths, is 50% too high. This necessarily means that the estimates of tCFR and sCFR they derived from it are too high by the same proportion.”
Worldometer now says 13 deaths, so it looks in line with the *case* fatality rates originally used by the Imperial folks. It was helpful of Nic to put up this analysis.
The Diamond Princess is not representative, Lombardy skews older, and Lombard cities + NYC hospitals were hit hard. But the numbers have me convinced that IFR must be higher than 0.17 % if you let it run rampant in the UK or US. 1% with a range still seems realistic but I don’t know enough to have a strong position. The Ioannidis confidence intervals looked messed up though.
Dhogaza, No scientist makes only correct predictions. Your’s is a meaningless observation. I’m more thinking of his Diamond Princess study (I think in early March as well) which has very similar numbers to the Santa Clara study. And yes, he took into account that more people might die, essentially doubling his numbers. Using those IFR’s excess mortality is not 10,000. It’s more like 200,000 if everyone is infected. He must have been assuming that only about 5 million would be infected. If you presented the context people could evaluate the claim accurately.
Mark, There’s a serious problem with doing a raw IFR for the Diamond Princess. The passengers were much older than the general population. What Ioannidis did was to project the age based IFR’s onto the general US population. That seems the right thing to do. I’d be shocked if Imperial reported the raw IFR without pointing out how it was so skewed.
> You are quoting Gelman out of context.
That’s untrue, David. I’m quoting the main conclusion from his analysis of the so-called Stanford study, to which John participated, a study that does not rest on any flag, Italian or otherwise. Also, we both know full well that your “every competent epidemiologist knows full well” is more than unsubstantiated.
If you’re to spam this thread, try to use proper citations.
“dpy6629 says:
May 10, 2020 at 3:59 am
I see that Schmidt, someone with no knowledge of epidemiology, attacks an expert with a very strong track record.”
says dpy6629 who has always been respectful of the expertise of those with strong track records in climate science…
“Picking out one example of a controversy about one of a prominent scientists papers is meaningless.”
#ButButMBH98*
* don’t worry not going to say more about it than that.
Joshua,
You’re right, of course. What I was getting at is the difference between attacking an individual, and attacking an entire research field. I think the former is easier, or more effective, than the latter, even though they would probably do the latter if they had to.
“In the conclusion of that blog post, he says he has no idea if the result is right or not, and that Ioaniddis and coauthors are the experts. He is just complaining about lack of adequate supplementary data about the testing method.”
That obviously isn’t a correct interpretation as Gelman identifies specific flaws and unequivocally states that the authors *did* make mistakes “I’m serious about the apology. Everyone makes mistakes. I don’t think they authors need to apologize just because they screwed up. I think they need to apologize because these were avoidable screw-ups. They’re the kind of screw-ups that happen if you want to leap out with an exciting finding and you don’t look too carefully at what you might have done wrong.”
Now you can get the right answer for the wrong reason (or using unreliable reasoning), and I think Gelman might not be questioning the result, but he is clearly very critical of the reasoning. But he is clearly doing a lot more than complaining about the lack of supplementary data.
He also doesn’t say “no idea” – perhaps you should give a direct quote to support that?
Hilarious, moa.
Just about everything that followed your claim to follow the evidence was untrue. Old Duane would be cheering from his grave.
OK not hilarious. Sad.
The amazing thing is how politically counterproductive attacking the scientists is likely to be in the UK for people who hate lockdowns: there is no way there will be a let-it-rip strategy so weakening the lockdown just makes it longer and more damaging.
At this point the UK public is starting to wake up to the fact that their nation is not doing well by comparison. Sitting in isolation while some others in Europe go on summer holiday is not going to be a happy period. Even the ones who didn’t want to play by the EU’s rules still wanted to play on their beaches.
I’m still astonished by how well Oz is doing in comparison (and note that the conservatives are in charge federally). There may now be no new cases in some states.
Also, this is what it looks like when a country knows what it is doing:
https://www.covid.is/data
Having once lived in Sydney, NSW, Australia for 9 months, yes. The am impressed with how well the Australians are handling COVID-19.
And welcome back, dpy.
You do have a talent for demonstrating the point of ATTP’s posts. But not in the way you think you are.
You should read Gelman’s other posts. That one was gentle. Ioannidis’s paper was one of the crappiest pieces of statistical analysis I’ve seen on the topic. A detection rate that equals the false-positive rate and somehow fails to include zero in the infection-rate uncertainty bounds. Then a PR blitz that pushes the other end of the uncertainty range. A population that is under-represented in the main demographic factors predicting fatality relative to the rest of the USA, and corrects for other things but not demographics (4% of the most vulnerable vs. 14% IIRC – hey, what’s 0.37 x 14 / 4?). The only crappier one was the paper on viral transmission through various types of face mask, which made the Challenger error of coding not-detected as zero when it was obvious that most of the detections were within an order of magnitude of the detection limit and the detection limit was high (based on the non-detection rate of known infected mask-free control subjects and high minimum value for the number of viral particles detected).
I’ve previously linked to a study comparing the age-stratified Diamond Princess death rate to China which found 0.5% IFR (including asymptomatic cases in the denominator). Estimating the infection and case fatality ratio for coronavirus disease (COVID-19) using age-adjusted data from the outbreak on the Diamond Princess cruise ship, February 2020. That was about a 50% downgrade of the Chinese 1%, because the DP cohorts were half as likely to die as their equivalent Chinese cohort. I speculated that that may be because wealthy cruise ship passengers who are up for a 10,000 mile flight and medical insurance are certainly wealthier and probably healthier than retired farmers or factory workers living on a meagre pension.
But, as I’ve also said on previous threads, playing with 1% IFR, 2%, 0.5% or 0.3% is angels dancing on a pinhead. To make a policy difference it has to be 0.1% with a vaccine, because then it’s like flu with only the unvaccinated low-risk cohorts and those whose vaccination didn’t take are infected. And well below 0.1% without a vaccine, ideally 0.01%. But if it’s as low as that we might as well give up on herd immunity because there are numerous places with more than 100% infected. Which means infection doesn’t confer immunity, other than to corpses.
Go Iceland! IFR 0.56% (with two still in hospital so it could rise to 0.67%, or a bit more if some of those in quarantine take a turn for the worse). Quelle surprise.
Test, trace and isolate works. Plus de surprise. And what highly commendable openness and clarity. Really nice webpage too.
And about half of those infected were not in quarantine when tested so presumably asymptomatic. Encore plus surpris.
I love it when a consensus comes together.
One thing distinguishes a lot of the countries that had an effective response (good job, Iceland) was that a large fraction of their cases are related to foreign travel (and they know this because they traced them). That means mostly younger folk. Respond early, and take serious measures, and you reap the rewards both in health and economic terms.
Icelandic hammer solution >> Thanos solution.
David –
> There is also the issue that the number of studies now is large enough that’s it’s unlikely all them are biased in the same direction.
They’re all in hotspots.
Let’s take the study in Chelsea, MA. You’ve mentioned that study before. You indicated it prives a high infection rate, a large denominator.
They estimated a 31.5% infection rate in Chelsea. Chelsea has 40,000 people. Right now, some 124 people from Chelsea have died from COVID (a number that’s sure to go up). You do the math.
There is also the issue that the number of studies now is large enough that’s it’s unlikely all them are biased in the same direction.
Oh, and the German study, in another hotspot, in a country with better outcomes than the US, in a town with a slightly lower mean age than Germany overall (I don’t know about other important variables of representativeness) ?
> However, some of the individuals still may have been acutely infected at the end of the study acquisition period (April 6th) and thus may have succumbed to the infection later on. In fact, in the 2-week follow-up period (until April 20th) one additional COVID-19 associated death was registered. The inclusion of this additional death would bring up the IFR from 0.36% to an estimated 0.41% [0.33%; 0.52%].
This is why you need to wait for better data. Respect the uncertainty.
Anders –
> What I was getting at is the difference between attacking an individual, and attacking an entire research field. I think the former is easier, or more effective, than the latter, even though they would probably do the latter if they had to.
OK. Gotcha.
Although I’ll point out that those who are ideologically motivated and conspiratorially predisposed (I won’t mention any names or screen names, but I think we all can point to two right now) attacking a group isn’t at all a deterrent.
David –
> I urge always writing the integer to the left of the decimal point even if that integer is zero.
Will do. Thanks. If I were smarter I would have thought of that myself. Especially since auiocorrect on my phone keeps confusing decimal points with periods.
David –
Respect uncertainty.
Santa Clara?
A hotspot.
Barcelona?
A hotspot.
NY?
A hotspot.
LA?
A hotspot.
Miami-Dade?
A hotspot.
Gangelt, Germany?
A hotspot
Hmmm. Maybe there’s a pattern here?
Here’s the results of a recent meta-anslysis:
> After exclusions, there were 13 estimates of IFR included in the final meta-analysis, from a wide range of countries, published between February and April 2020. The meta-analysis demonstrated a point-estimate of IFR of 0.75% (0.49-1.01%) with significant heterogeneity (p<0.001).
Respect the uncertainty.
Joshua says:
“At any rate – the point being to respect the uncertainty, until we have better data.”
Why start now?
It is a bit late.
Plus it is more than the data,
Every Pandemic presents something novel so past experience does not guide future results.
What was that story about the fellow with the lion on the loose.
Sometimes you have to respect the uncertainty,
Sometimes you have to run.
05/10/20
Someone shows up and all of a sudden it is Groundhog Day.
But yes, to all those countries that did the right things from the get go and stayed the course. There are now literally dozens of those countries that did the right things.
And there are a few handful of countries that really scotched things up badly.
And then that one country, the US, that will continue to scotch things up badly throughout the rest of 2020.
Oh and what will the world do with all those excess aeroplanes?
David –
Some people argue that the same number will get infected irrespective of government interventions.
The corollary is that reaching that number slowly will cause less economic harm, and that the differential harm from shelter in place orders is unambiguously enormous as compared to a slower spread where some 50%? of the population gets infected.
That argument, of course, is easy to make but only if you fail to respect the enormous uncertainties involved. Conditional probability is hard
You might look at the economic impact in Denmark vs. Sweden as an example, but cross-country comparisons are fraught with uncontrolled variables.
There are plenty of reasons to believe that with building testing, tracing, and isolating infrastructure rather than just opening things up, the economic impact can be mitigated. And of course, there no reason why opening up and building thst infrastructure need to be mutually exclusive.
But where people want to be indignant and see petty tyrants to rail against, they will do so. One way that people deflect fear is to see themselves as victims.
And where people feel better about themselves by attacking scientists, they will do do.
And respecting uncertainty is hard.
Besides uncertainty, we should respect the number of beds:
https://www.cbc.ca/news/canada/montreal/montreal-hospitals-space-covid-19-1.5558118
Listen to epidemiologists all you want. But please, very please, stay safe. Those having to work in hot spots (like my spouse) will thank you. Your loved ones too. This is not a mild flu:
> Sometimes you have to run.
Harder to run when you’re in a coma, doc:
Ask you fellow doctors when was the last time they had a day off. They can thank your government for that:
https://www.wsws.org/en/articles/2020/03/19/doct-m19.html
Even without a vaccine, the virus is going to disappear:
dpy
the best evidence seems to show IFR’s between 0.12% and 0.4%
As Mark said above the *mortality* rate in several cities or regions is already being reported above this, let alone the IFR.
This highest rate in the uk is 0.14%
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19bylocalareasanddeprivation/deathsoccurringbetween1marchand17april#local-authorities
Nobody is suggesting that infection rates in London are approaching 100%.
One can only conclude that the “best” definition of “best evidence” is “evidence which agrees with dpy’s preferred conclusion”.
Short version: no surprise at dpy cherries, yet again.
If actually interested in IFR, recent and much awaited estimate from Germany of 0.37%
Click to access Streeck_et_al_Infection_fatality_rate_of_SARS_CoV_2_infection2.pdf
As with flatearthers, AGW deniers, Anti-vaxxers, 911 twoofers and Covid19 deniers
There are essentialy two types
Those that sell the T-shirts, and those that buy the T-shirts
Its as old as the hills
VTG –
As I posted above, that German study is already up to a 0.41 IFR.
Thanks Joshua, missed that
> If actually interested in IFR
I’m more interested in the kind of inferences one can make with claims such as “the best evidence seems to show IFR’s between 0.12% and 0.4%.” Notice David’s first paragraph here:
[DY1] Well, We have no idea if Ferguson was telling the truth but I’m willing to give him the benefit of the doubt. The problem here is that his science was wrong and his track record seems to be to mostly err on the alarmist side.
In response to the observation that John’s 10K was a bit incorrect, here’s his response:
[DY2] No scientist makes only correct predictions. Your’s is a meaningless observation. I’m more thinking of [..]
followed by a squirrel. On the one hand there is a pretaeritio about truthfulness and #ButAlarmism. On the other, there is errare humanum est.
I wonder why David’s tricks can be identified using latinisms. Could it be because non nova, sed nove?
dpy6629 | May 10, 2020 at 12:37 pm |
Josh, It’s getting very boring checking out your pseudoscientific links. The first one to HealthLeaders is a bad study using top liner case numbers. It’s results are meaningless because the more you test, the more cases you find.
With respect, I would suggest looking for actual scientists doing high quality science, not “journalist” reports using meaningless numbers.
Joshua | May 10, 2020 at 12:58 pm |
Your comment is awaiting moderation.
David –
> With respect, I would suggest looking for actual scientists doing high quality science,
With respect, the study [written about in Health Leaders] was published in Health Affairs:
>. Health Affairs’ Impact Factor Reaches 5, Ranking First Among Health Policy Journals
https://www.healthaffairs.org/do/10.1377/hblog20160620.055444/full/
I’ve long suspected that David is a Poe.
Willard,
Indeed. Dpy – semper idem. The IFR paper is wasted on him, as it dies not age with his conclusions.
More evidence that David is a Poe?:
> dpy6629 | May 10, 2020 at 2:38 pm |
Your reference is worthless. From the KEY TAKEAWAYS
“The researchers looked at 116 counties in 33 states and found 40,835 confirmed cases and 1,620 confirmed deaths through April 20.Asymptomatic COVID-19 patients who recovered with no symptoms were not counted in the data, which could have skewed results.”
That it was published in a journal is just you making an argument from authority.
——
So that was after I clearly stated multiple times that the article refers to a *symptomatic” fatality rate. I clearly indicated that the IFR-S, at 1.3% should be reduced by 20% or 50% or whatever asymptomatic rate you want to use. The Princess Diamond asymptomatic rate was around 20%, but use 50% and you still get an IFR much higher that the upward bound of the range David prefers.
The article which linked the study also discussed this, as does the study itself.
The probability that David is a Poe is increasing exponentially with each of his comments.
I hope he comes back to clear his good name.
Here’s an extended quote from Gelman’s original post from near the end:
“I’m not saying that the claims in the above-linked paper are wrong. Maybe the test they are using really does have a 100% specificity rate and maybe the prevalence in Santa Clara county really was 4.2%. It’s possible. The problem with the paper is that (a) it doesn’t make this reasoning clear, and (b) their uncertainty statements are not consistent with the information they themselves present.
Let me put it another way. The fact that the authors keep saying that “50-85-fold” thing suggest to me that they sincerely believe that the specificity of their test is between 99.5% and 100%. They’re clinicians and medical testing experts; I’m not. Fine. But then they should make that assumption crystal clear. In the abstract of their paper. Something like this:
We believe that the specificity of the test used in this study is between 99.5% and 100%. Under this assumption, we conclude that the population prevalence in Santa Clara county was between 1.8% and 5.7% . . .
This specificity thing is your key assumption, so place it front and center. Own your modeling decisions.”
Gelman had another post on the second version of the paper which concludes that the second version is an improvement. I don’t see that this really amounts to a definitive criticism and its certainly a far cry from Willard’s original selective excerpt.
But this is mostly irrelevant because there are now 3 studies that give much the same conclusions. Santa Clara, Los Angeles, and Miami Dade.
DPY,
Links?
Josh, Your “study” uses “case” numbers and not infection numbers. It doesn’t mean much. Case numbers are completely dependent on the level of testing deployed in these counties.
> I don’t see that this really amounts to a definitive criticism and its certainly a far cry from Willard’s original selective excerpt.
Of course you don’t, David. Here’s the excerpt, this time with its textual function:
https://statmodeling.stat.columbia.edu/2020/04/19/fatal-flaws-in-stanford-study-of-coronavirus-prevalence/
You’re saying that Andrew’s own summary is a “selective excerpt.”
Do engineeers working for one of the biggest military defense firms in the world ever learn to read?
Herd immunity. No vaccine. Lol.
> Gelman had another post on the second version of the paper which concludes that the second version is an improvement.
That’s one way to put it [NB]. Another is to “selectively quote” Andrew’s own tl;dr from the most recent study:
https://statmodeling.stat.columbia.edu/2020/05/01/simple-bayesian-analysis-inference-of-coronavirus-infection-rate-from-the-stanford-study-in-santa-clara-county/
My own emphasis.
***
[NB] – I will simply note:
https://statmodeling.stat.columbia.edu/2020/04/30/updated-santa-clara-study-of-coronavirus-infection/
Funny how selective auditors are regarding data and code.
Willard –
In fall fairness, FWIW I recall Andrew somewhat walking back that “they owe us an apology” comment…not completely, but somewhat. I looked for it a bit but I can’t find it now…
As a backdrop to your general discussion of the broad topic of scientists and policymakers, the best book out is by David Michaels, “the Triumph of Doubt: Dark Money and the Science of Deception.”
Michaels writes with a lifetime of experience of being the head of OSHA during the Obama years, a long-time academic, and a gifted and accessible writer who has had to endure the horrors of engaging with industry jerks, prostituted industry scientists, moron industry judges, and lowest of the morons, Republican politicians.
What a wonderful system – dupes, sycophants, deniers, liars, con men, all lavishly funded by killer corporations, and yet you aver that “the responsibility for making decisions lies with policy makers, not with scientists.” That’s the recipe for death via mass murder, as we can now see clearly.
David –
> Josh, Your “study” uses “case” numbers and not infection numbers. It doesn’t mean much. Case numbers are completely dependent on the level of testing deployed in these counties.
The did not calculate a case fatality rate. They calculated a fatality rate among symptomatic cases. And anyway, the rate of people with symptomatic cases who die does not depend on the level of testing employed.
Why is this kind of stuff so difficult for you to understand?
It’s similar to your inability to understand the problem with going from an *infection rate* estimate for a a non-representative (and non-random, likely self-selection biased) sample from Santa Clara, and jumping to extrapolating more broadly a *infection fatality rate” with populations that are much, much different in many important respects.
It’s really perplexing why you have so much trouble with this.
notabilia,
Surely, in most of our societies what I said is a truism (we elect people, who represent us, and who make decisions)? I don’t really see some alternative that would be preferable. What I’m getting at is that we shouldn’t let our policy makers off the hook but allowing them to blame the scientists (or any expert advisers) when their decisions are unpopular, or end up being the wrong thing to have done.
No rush, Joshua. Take your time. Meanwhile, Andrew is running a post on Ferguson’s case, more specifically a National Review reporter who echoes David’s tendentious remarks.
First comment from the thread is from our own James:
https://statmodeling.stat.columbia.edu/2020/05/08/so-the-real-scandal-is-why-did-anyone-ever-listen-to-this-guy/#comment-1331855
The real scandal is why did anyone ever listen to climate contrarians.
Willard –
I gave up trying to find it – it might have been in the comments. I could be wrong, but basically my recollection is that in retrospect he felt that saying they owed an apology was a bit strong – even if he did think that they made errors that could have relatively easily been avoided.
Andrew specifically said that he thought that my reaction – when I said that I thought it broke basic scientific principles to jump from infection rates with a non-random, non-representative sample to extrapolating a broadly applied fatality rate – was not something he agreed with. He said something along the lines of “statistic are hard.” I still don’t get how he thinks that kind of extrapolation is justifiable, and I couldn’t get him to explain it to me – but of course he’s smarter than I am.
9th “Joshu” on the page gets me this:
https://statmodeling.stat.columbia.edu/2020/04/19/fatal-flaws-in-stanford-study-of-coronavirus-prevalence/#comment-1307481
I think the apology for being sloppy still stands. He has not taken issue with their political ploys, like going on Fox News to say it was not more deadly than the flu.
Willard –
Yeah, it was after that. I tried searching for “Andrew says” and didn’t find it. It may be buried in one of the subsequent posts on related topics. Sorry. I know you don’t like it if someone just says “I remember that…” and doesn’t provide the quote. I may have “misremembered.”
I pushed him on the PR political campaign from Iaonnidis et al., but Andrew wouldn’t bite. I had the distinct impression that he was avoiding direct criticism of John. There were a couple of time subsequently when peooke targeted John specifically, Andrew pointed out the 17 other authors earlier in the list. I repeatedly raised the issue of the “just like the flu” crap – especially since it was based on a bogus extrapolation, but no dice. And I repeatedly pointed to John’s selective treatment of uncertainty in that video that David posted. No dice.
Oh well.
At any rate, it was disappointing for me to see John peddling crap and playing rhetorical games. I kind of thought he was one of the good guys. I’m trying to not get too cynical about it.
“But this is mostly irrelevant because there are now 3 studies that give much the same conclusions. Santa Clara, Los Angeles, and Miami Dade.”
there is WAAY more than that and much better designs than Santa clara.
Colorado, Arizona, New York, Stanford Hospital ( complete Serology of entire staff
and patients, super reliable test.) Miami, The mission district in SF. None of this heavily reported by MSM.
All pointing in the same ballpark.. ( but its a big park)
take Arizona
Population 7.3M
Serology 3.4% positive
Estimated infected: ~250,000
Postive cases: 11,200.
Got that? Arizona has tested 27,000 people for antibodies, 3.4% positive.
That would indicate ~250K have had the virus But only 11K have showed up
for PCR testing because of symptoms.
So like 20X times more people get the disease than are reported
Total Deaths 536
536/250,000 ~.2 %
But.. there are another 1000 or so of the high risk group still in the hospital.
so 1500/250000 = .6%
Arizona has great data. Even listing cases by setting types.
Assisted living if leading the pack and other congregate settings.
hospitals prisons nursing homes.. all big.
testing will ramp to 250,000 people. staff, students, etc.
Misson district testing in SF was very interesting as well.
Positive Serolgy Indicates actual cases in SF to be ~19K
Reported cases 1900. 10X
deaths: 34
do the math.
Miami. Population 400,000 6% positive.. 24K cases, 8000 reported. 3X
However. there are many many buts, but but but
kinda funny that there are some serology deniers
“DPY,
But this is mostly irrelevant because there are now 3 studies that give much the same conclusions. Santa Clara, Los Angeles, and Miami Dade.
Links?
Arizona
https://www.azdhs.gov/preparedness/epidemiology-disease-control/infectious-disease-epidemiology/covid-19/dashboards/index.php
then google
serology miami
serology colorado
serology mission district.
For the Stanford hospital numbers, you have to watch the “grand rounds” live stream
they are testing all staff and patients
Big trial started in Michigan
https://clinicaltrials.gov/ct2/show/NCT04349202
I am sure there will be buts
Thanks Steven, For Arizona, taking the death number from 14 days after the mean test date is what Ioannidis et al did. Some of those who are seriously ill were infected after the test mean date.
Another PS from Gelman.
“Let me again emphasize that “not statistically significant” is not the same thing as “no effect.” What I’m saying in the above post is that the information in the above-linked article does not provide strong evidence that the rate of people in Santa Clara county exposed by that date was as high as claimed. Indeed, the data as reported are consistent with the null hypothesis of no exposure, and also with alternative hypotheses such as exposure rates of 0.1% or 0.5% or whatever. But we know the null hypothesis isn’t true—people in that county have been infected! The data as reported are also consistent with infection rates of 2% or 4%. Indeed, as I wrote above, 3% seems like a plausible number. As I wrote above, “I’m not saying that the claims in the above-linked paper are wrong,” and I’m certainly not saying we should take our skepticism in their specific claims and use that as evidence in favor of a null hypothesis. I think we just need to accept some uncertainty here. The Bendavid et al. study is problematic if it is taken as strong evidence for those particular estimates, but it’s valuable if it’s considered as one piece of information that’s part of a big picture that remains uncertain. When I wrote that the authors of the article owe us all an apology, I didn’t mean they owed us an apology for doing the study, I meant they owed us an apology for avoidable errors in the statistical analysis that led to overconfident claims. But, again, let’s not make the opposite mistake of using uncertainty as a way to affirm a null hypothesis.”
It’s odd that people here are focusing on criticisms of inadequate data and method info in the paper while ignoring the fact that the criticisms are from a person who is not an expert and admits that the authors are the experts.
Steven –
> Got that? Arizona has tested 27,000 people for antibodies, 3.4% positive.
That would indicate ~250K have had the virus But only 11K have showed up
for PCR testing because of symptoms.
So like 20X times more people get the disease than are reported
Total Deaths 536
536/250,000 ~.2 %
But.. there are another 1000 or so of the high risk group still in the hospital.
so 1500/250000 = .6%
—————————————-
I went to the link. I couldn’t find how people are selected for/get the test, particularly if they aren’t symptomatic.
BTW –
Saw a recent flyer for SF (GetTestedSF). – don’t know if that applies…
Requirements are: “All essential workers can get tested regardless of symptoms. For anyone else, you must have at least one of the COVID-19 symptoms….”
“It’s odd that people here are focusing on criticisms of inadequate data and method info in the paper while ignoring the fact that the criticisms are from a person who is not an expert and admits that the authors are the experts.”
Where did Gelman argue that he’s not an expert in statistical analysis?
Anyway, the problem here is the push to set national policy based on serology results that are quite uncertain. Not to mention that there is no data on what level of antibodies are required to impart immunity, and the serology tests don’t get us that information.
David –
> It’s odd that people here are focusing on criticisms of inadequate data and method info in the paper while ignoring the fact that the criticisms are from a person who is not an expert and admits that the authors are the experts.
I don’t need Gelman’s criticism to know that extrapolating from a non-random, non-nationally representative sample (not by a long shot) to offer a broadly based fatality rate is bad science. I don’t need Gelman to know that their sampling method was likely to have a problem with self-selection bias. I don’t need Gelman’s criticism to know that Ioannidis should not have used the Santa Clara study to as a basis for saying that COVID-19 is like the seasonal flu.
But it seems that you’re still stuck on understanding what random and representative samples are.
Other data.
Stanford is testing blood donors but not reporting results
France reports 3% from blood donors
Click to access 2020.04.21.20068858v1.full.pdf
In the US the government is
A) claiming a huge effort (not)
B) taking their time
https://www.sciencemag.org/news/2020/04/unprecedented-nationwide-blood-studies-seek-track-us-coronavirus-spread
Stanford in the news
if yu want to watch the doctors at Stanford talk weekly.. go to youtube “Stanford grand rounds”
SM:
“kinda funny that there are some serology deniers”
Pointing out that the available data has uncertainties, that the false positive problem could be worse than stated and that this impacts studies with a very low percentage of positive results, and thus far there’s no data on what level of antibodies are required to impart immunity and that it is premature to set policy (“open up the country!”) does not make one a “serology denier”.
> Misson district testing in SF was very interesting as well.
Positive Serolgy Indicates actual cases in SF to be ~19K
Reported cases 1900. 10X
deaths: 34
do the math.
Mission district isn’t representative. As I recall, something like 45% of those tested were white and something like 95% of those who tested positive were Latinx. But then, the fatality rate among Latinx should be quite high.
All in all, tough data for learning much.
I noticed first you said “”Mission District testing” but then gave the case numbers for SF?
dky:
And Gelman also says in his post that
“The Bendavid et al. study is problematic if it is taken as strong evidence for those particular estimates”
You have stated in various places that the IFR is 0.12%-0.31%, as though it is established fact. If you’re going to quote Gelman you might heed his warning.
> It’s odd that people here are focusing on criticisms of inadequate data and method info in the paper while ignoring the fact that the criticisms are from a person who is not an expert and admits that the authors are the experts.
It’s odd that David would interpret Andrew’s I’d mostly call them a bunch of doctors and med students as admitting that the authors are the experts.
But what do I know about how aeronautic engineers are being taught to read.
Josh, Your reference does not calculate an IFR. The “asymptomatic” statistics are even squishier than most things in this field. There are a continuum of symptoms and many people consider a minor cough to not be significant enough to contact the medical system for example. One brother of a coworker is an MD on the east coast who is about 30 years old. In February, he had a minor cough and low grade fever for 3 days. He thought nothing of it. In March he volunteered in a NY hospital and was tested. He was seropositive. Everyone agrees that this is the usual coarse of covid19 in young and healthy individuals. Your paper also relies on modeling, not on actually testing statistics.
It’s a weak paper and I’m surprised you keep bringing it up as if it means much.
paucity of data on plasma treatments
https://sci-hub.tw/10.1002/jmv.25961
5 studies. looks like 0 mortality, but tiny numbers
David –
> Josh, Your reference does not calculate an IFR. The “asymptomatic” statistics are even squishier than most things in this field.
You keep getting this wrong. Did you even read the paper?
It wasn’t an “asymptomatic” statistic. You have it completely backwards.
They called it an IFR-S. The “S” stood for symptomatic. They calculated a fatality rate for symptomatic people. That’s a rate. It doesn’t depend on the number of people they identified as symptomatic. It’s the number of people they identified that died. From that, you can use whichever number you want to determine how many more people there are that are asymptomatic vs. symptomatic.
> There are a continuum of symptoms and many people consider a minor cough to not be significant enough to contact the medical system for example.
Do you know what definition they used in the study? Did you read the study?
VeryTallGuy, the uncertainty that this study does not take into account is the number of people who died. That is just 7. It could just as well have been 5 or 10. If you also take that uncertainty into account the Infection Fatality Rate could also be above 1%.
Like all such studies you have the sampling problem that not everyone participates and people who had or know cases are likely more willing to participate because they would like to know themselves where they are affected.
The range of the meta-study Joshua cited sounds very reasonable to me, it was also the range virologist Christian Drosten mentioned last week (he is an expert for emerging viruses and Corona viruses and developed the WHO test): 0.5 to 1%.
(I translated some of his regular public radio interviews into English, in case anyone is interested in a reliable scientific source on Corona: https://variable-variability.blogspot.com/2020/03/german-virologist-Christian-Drosten.html )
Steven –
> “kinda funny that there are some serology deniers”
My recollection is that you have written quite a bit about how counterproductive using the term “denier” is. Causes a backlash, doncha know.
But at any rate, I don’t care. So what is a serology denier, anyway? What’s the definition?
Dhog, As Steven points out there is a growing body of evidence. The focus on this one particular study does nothing to invalidate the growing body of rather strong evidence. The Santa Clara study is consistent with that body of evidence. The authors are continuing to strengthen their data on the testing specificity. They are experts in the field with a long track record that is quite good. I guess some people just have trouble accepting good news. We should all want the news to be good and scientifically correct.
One more time Josh. The study does not calculate an IFR and so is not evidence on this issue.
“Pointing out that the available data has uncertainties, that the false positive problem could be worse than stated and that this impacts studies with a very low percentage of positive results, and thus far there’s no data on what level of antibodies are required to impart immunity and that it is premature to set policy (“open up the country!”) does not make one a “serology denier”.
That will be a good test to apply across fields of inquiry. haha. especially the argument that the lack of data makes it premature to set policy.
BTW, I dont think serology should be used to set policy, rather some of the “scary: scenarios
need to be retired.. they served their purpose.
And yes, the low positive rates ( combined with test accuracy) remains an issue.
Nevertheless I do find it shocking that the CDC is moving at a snails pace. The director
struck me as totally inept leader.
I loved this lady
David –
> > Josh, Your reference does not calculate an IFR. The “asymptomatic” statistics are even squishier than most things in this field.
This is also pretty interesting because you’re on here telling us that you know with a lot of certainty what the fatality rate is. And you base that on estimates (using models, of course) of asymptomatic cases in contrast to identified cases.
And I’m the one who keeps saying you should respect the uncertainty.
And then you come back and say that the “asymptomatic” statistics squishy.
Do you not even realize that the all those studies you keep mentioning, including the Santa Clara study, are largely based on modeling based on “asymptomatic” cases? Wow.
David – let me ask you straight up. Are you a Poe?
David –
> The focus on this one particular study does nothing to invalidate the growing body of rather strong evidence. The Santa Clara study is consistent with that body of evidence.
Almost all of which thus far was conducted in hotspots, and all of which is fundamentally based on data that you just called “squishy.”
David –
> One more time Josh. The study does not calculate an IFR and so is not evidence on this issue.
Yes. You keep saying that, along with making a long list of errors. And I keep correcting those errors and explaining to you what it actually does. And of course, you ignore all of that and just keep restating the same mistakes.
Anyway, Steven –
I await your responses regarding the testing in protocol in Arizona, about the combination of “The Mission District” and SF data, and how you define “serology denier.”
“I noticed first you said “”Mission District testing” but then gave the case numbers for SF?”
ya sorry.
I just found the by zip data.. yu want it?
Mission district: population 73000
Cases: 283
Infection rate from serology ~2%
expected cases ~1460
deaths: 0
> I just found the by zip data.. yu want it
I don’t really care about the details. I’m more interested in the overview.
0 deaths. Wow. In a largely Latinx community, with a lot of poor Latinx, except the rich white hipsters and Googlers. What’s up with that?
To go one level higher. It may be interesting to nerd out on the IFR estimates, but whether it is 0.1% or 1% does not really matter that much for policy. In both cases you would need similar measures to avoid the hospitals being overrun, because once they are overrun the mortality rate would be a few percent.
That the flu has an 0.1% IFR is irrelevant is not comparable to COVID-19 even if its IFR were 0.1%. People get the flu over their full life span (thus no hospitals overrun), while now everyone gets it in a few months (if we would not take any measures or open up too early) and thus have overrun hospitals.
“Dhog, As Steven points out there is a growing body of evidence. The focus on this one particular study does nothing to invalidate the growing body of rather strong evidence. The Santa Clara study is consistent with that body of evidence. ”
All of the low prevalence data ( where the serology is low single digit ) should be viewed
with EXTREME caution, because of false positives.
take the Mission district as an example. a test with a false rate of 2% will…
guess what? find false positives. DOH!
the issues are WHY do we want to do serology.
1. To find more Plasma donors.
2. To understand the profile of the people who do not get symptoms (not being done in all cases)
3. To “correct” as best as possible some of the scarier scenarios.
But no amount of serology testing will turn this into the flu, and none will answer the
question of how much risk is acceptable to whom.
‘I await your responses regarding the testing in protocol in Arizona, about the combination of “The Mission District” and SF data, and how you define “serology denier.”
Protocal in Arizona? I will look it up.
I am currently looking at the protocol for collecting tree rings..
haha.
I’d add a #4 – at least at the point where immunity is more certain…to ascertain when people are safe to walk around, be with more vulnerable people.
No saying how long that will be… so much depends on that.
To come back to the original post: “There’s been some discussion about scientists being attacked for telling the truth. I do, of course, think that this is a real issue, but I also find myself somewhat frustrated by all of this. It’s hardly surprising to anyone who is aware of what has happened in the climate context.”
I like it, to be honest. Epidemiologists and virologists have the right to be mad, they should be mad. The disgusting barbaric behaviour of the anti-science crowd is not acceptable behaviour. While climatologists tend to say you just need a thick skin, I like it that they are justifiably mad and that the population agrees that the behaviour of the climate “sceptics” is not acceptable.
Why they did not expect this? How long ago is the last pandemic? I do not know how it was in Australia, England and America, I presume you have suffered because of Murdoch for a longer time, but when I was young newspapers aimed at writing things that were relevant for their paying readers. The letters to the editor could be a bit wilder, but were still expected to contain actual arguments, to be mostly truthful and use somewhat decent language.
Conspiracy theorists, violent people and mentally deranged people were isolated at home. If they had an outlet it was with some drunk folks at their local bar. They were not organized by the moneyed interests who would like to define what is true as what serves their interests and not have those scientists with their “EXpEriMenTs, aRguMeNtS and cOmPutAtioNs” get in the way of profits.
Junior auditor Joshua
start here
https://www.sonoraquest.com/newsroom/posts/sonora-quest-laboratories-now-offering-covid-19-antibody-testing-in-arizona/
next time ask pretty please with sugar on it. Willard will get the joke
https://www.sonoraquest.com/sonora-quest-laboratories-now-offers-covid-19-antibody-testing/
using ELISA, Ig
Sensitivity 90%, Specificity 100. per the FDA
“I’d add a #4 – at least at the point where immunity is more certain…to ascertain when people are safe to walk around, be with more vulnerable people.”
the ButImmunity people will say it is never safe.
There will always be a but. ButMutationMayHappen, ButSecondWave
there will always be an argument to stay closed and isolated. no one in government
and no medical professional association or group will ever tell you, you are safe.
They will never ever as group deliver a consensus message that it is over or safe.
It is not in their interest. They too have motivated reasoning.
well, until more hospitals fail from lack of patients willing to go in for elective surgery.
Important knowledge gap
Click to access 2020.04.27.20081893.full.pdf
While herd immunity is expected to require 60-70% of a homogeneous population to be
119 immune given an �! between 2.5 and 3 (2, 3), these percentages drop to the range 10-20% for
120 CVs between 2 and 4. Therefore, a critically important question is: how variable are humans in
121 their susceptibility and exposure to SARS-CoV-2?
Steven Mosher sez:
“Nevertheless I do find it shocking that the CDC is moving at a snails pace.”
I don’t. Two words. Small Hands.
In my homeland that is a shlthole of a country currently under a shltstorm of a pandemic with a dipshlt of a POTUS, aka Small Hands, who will disappear the virus away without a vaccine (I kid you not), who fires or silences anyone who disagrees with his bowel movements, I don’t expect the CDC or any other federal government scientists have the capability to simply do their jobs in a timely manner, not when they are being told what to say out of fear for their own jobs or livelihoods.
Or just call shlt what it is, political diarrhea from dipshlts.
” and how you define “serology denier.”
by the selectivity of their buts and how they USE uncertainty to promote their desired
policy.
example: early on people who wanted a lock down used uncertainty data from China
without any buts. They ignored uncertainties about whether people would actually
follow policies. they expressed doubts about effective mask use without expressing doubts
about effective hand washing. They expressed no doubts about lockdowns being more
or less effective as a function of density or housing arrangements. They expressed doubts
about outdoors transmission being low when all the data said otherwise.
And now they use doubt about serology. Like saying you cant compare countries.. forgetting
that the early modelling all assumed china was typical.
Its not so much the existence of the but. its about the inconsistency of the response to uncertainty
and the use of uncertainty to prolong a state they find more comfortable than change.
The funniest but is the “not a controlled experiment” but.
here is the thing. we will never have that.
@-“Surely, in most of our societies what I said is a truism (we elect people, who represent us, and who make decisions)? I don’t really see some alternative that would be preferable.”
Societies in which we elect people, who represent us, and who make decisions are the lucky ones, and few and far between.
In most democracies we elect people who make decisions in accordance with those that provided the most funding that financed their election campaigns.
Or who spend the most on lobbying (bribing) the executive branch, or in the most mature democracies, went to the same school and universities.
The primary purpose of democracy is to provide a facade of legitimacy to the underlying policy choices of the economic interests.
That is why there is such a push-back on the scientists when they provide ugly facts that undermine the prevailing interests in maintaining BAU.
> whether it is 0.1% or 1% does not really matter that much for policy
A bit like sensitivity matters. It’s as if the world was rediscovering a decade of ClimateBall in a month. Anyone who spends days arguing about death reates should consent in ceding their right to a respirator or a dialysis machine.
Most people I’ve seen debating these things just don’t have no idea what hospitals are like these days. Nobody wants to lockdown. But something needs to be done to lower the numbers ASAP.
In contrast to AGW matters, we know what needs to be done to get out of the lockdown:
[Playing the ref. -W]
On Steven Mosher wrote on May 11, 2020 at 12:53 am this as a statistic for Arizona:
Total Deaths 536
536/250,000 ~.2 %
I am surprised that some are making a rather serious mistake when trying to properly calculate the death rate from Covid-19. The total number of deaths from this virus are far higher than the “official” count. The numerator is way too low – very many more have died in Arizona than the “official” count of about 536. If we are to do a statistical estimate for the denominator, we must do the same for the numerator – but it was not done here.
Did Arizona COVID-19 deaths start in February?
https://www.abc15.com/news/local-news/investigations/how-many-arizona-covid-19-deaths-are-uncounted
Quote:
“So far, through 16 weeks, there’s been 1,135 deaths classified in the category. The previous average for an entire year: 1,307.
“This is a category in which only 20 or 30 deaths are assigned each week,” said Garrett Archer, ABC15’s data analyst. “In the last several weeks, we’ve seen this explode.”
Starting in February, the cases in this category began to sharply rise, reaching a high-point of 113 deaths in the eleventh week this year.
Clark believes these likely indicate uncounted COVID-19 deaths.
“The timing I think is perfect,” he said.
Clark later added, “I predict that category is going to come back down to what it was in the past. And if you do testing, you’re going to get a new COVID-19 category that is going to suck up most of that.”
The fact that people are dropping dead like flies at home or otherwise outside the hospitals due to “mysterious” causes – “mysterious” because their bodies are never tested for the virus – is just a coincidence, and has nothing to do with Covid-19? Nonsense.
People need to keep in mind that even if the true mortality rate were even something as low as, say, 0.6%, that would still be on the order of an entire order of magnitude more deadly than the typical flu virus of 0.1%. To see this, translate into a fraction with 1 as the numerator. A 0.1% death rate means 1/1000 die, while a 0.6% death rate means about 1/167 die. The latter is well within being on the order of 1/10^2, while the former is on the order of 1/10^3. I personally use this to educate “skeptics” – they can see very clearly that 167 is much closer to 100 than 1000, and thereby see much better how much more deadly this virus is than than the typical flu in terms of orders of magnitude.
There is one massive cover-up by the conservative media going on. Here is a sample timeline of the brainwashing in progress, followed by the truth as to the very many dying because of Covid-19 but not being counted as such:
Death Toll Conspiracy: Why Conservative Media – And Soon, Possibly Trump – Are Doubting Coronavirus Mortality Figures
https://www.forbes.com/sites/mattperez/2020/05/10/death-toll-conspiracy-why-conservative-media-and-soon-possibly-trump-are-doubting-coronavirus-mortality-figures/#7aa5d3df57d5
US death toll could be double official figure, expert warns as thousands avoid seeking medical help over coronavirus fears
https://www.independent.co.uk/news/world/americas/us-coronavirus-real-death-toll-covid-29-cases-a9504911.html
Hidden Toll: Mexico Ignores Wave of Coronavirus Deaths in Capital
More than three times as many people may have died from Covid-19 in Mexico City than federal statistics show, according to a Times analysis
Global coronavirus death toll could be 60% higher than reported
https://www.ft.com/content/6bd88b7d-3386-4543-b2e9-0d5c6fac846c
Quotes:
“The extra deaths are most pronounced in urban areas with the worst virus outbreaks, and have completely overwhelmed reporting mechanisms in some. This is especially worrying for many emerging economies, where total excess mortality is orders of magnitude higher than official coronavirus fatalities.
In Ecuadors Guayas province, just 245 official Covid-related deaths were reported between March 1 and April 15, but data on total deaths show that about 10,200 more people died during this period than in a typical year – an increase of 350 per cent.
…..
In the Indonesian capital Jakarta, data on burials shows an increase of 1,400 relative to the historical average during the same period – 15 times the official figure of 90 Covid deaths for the same period.”
“Experts have warned of serious under-reporting of Covid-19 cases in residential facilities for the elderly, who are particularly vulnerable to the virus. “Very few countries appear to be testing people in care homes, staff and residents, systematically,” said Adelina Comas-Herrera, research fellow at the Care Policy and Evaluation Centre of the London School of Economics.
Even the much higher numbers of deaths in the pandemic suggested by excess mortality statistics are likely to be conservative, as lockdowns mean that “mortality from numerous conditions such as traffic accidents and occupational injuries possibly went down”, said Marketa Pechholdova, assistant professor of demography at the University of Economics, Prague.”
“The point is that here it just might, but we are mostly ignorant of the actual parameter values”
izen,
Fair point. However, that still doesn’t imply that we should simply pass on the responsibility to some unelected group; we should be doing things to reduce the influence of those donors and doing more to ensure that our elected leaders make decisions that are in our collective best interests.
Can I clarify what the whole argument with DPY is about. From what I’ve seen, the fraction of people who’ve already been infected is probably less than 10% of the population, and the IFR is probably bigger than 0.1%, but less than 1% (the kind of numbers I see popping up quite a lot are 0.3% to 0.4%). Do some disagree with this?
Everyone sensible saw what was happening in Italy, that this was in no way ‘just the usual flu’, and set about trying to make sure it didn’t happen where they lived. The really bright ones caught on a bit earlier.
Bergamo and NYC are what it looks like when control measures are poorly implemented; we haven’t seen what completely uncontrolled spread looks like, but I invite you to look at the the situation in Manaus.
Half-hearted control measures designed to ‘protect the economy’ or ‘safeguard personal freedom’, as well as causing a large number of unnecessary deaths, just prolong the pain. New Zealand will soon be back to near-normal. Sweden not.
I think that there are estimates of IFR from various studies roughly in the range 0.1%-1% (possibly somewhat higher too). dpy is insisting it must be at the low end of this range, and focusing only on carefully chosen US serology studies.
In reality, you should consider all the evidence together, and that leads to the lower end of this range being extremely implausible.
There are regions/cities where more than 0.3% of the population have died of COVID. So this essentially rules out the IFR being less than 0.3% (i.e it is probably much higher).
I think the main point of annoyance is the claim that if the IFR is 0.3%, the US may as well just let everyone get it now, because 1 million deaths isn’t so bad anyway. For some reason that causes a strong reaction.
thats about right attp. any way you cut it its a lot of people dead. i just looked at the random testing and serology plan fir the UK.
REALLY small and they dont plan on asking a lot of demographic questions or behaviorial questions. odd. seriuously id volunteer to be tracked completely and open source all my medical data. after all some poor fuckers are going to take a vaxx before its proven..some already have..hands up chaps..
“There are regions/cities where more than 0.3% of the population have died of COVID. So this essentially rules out the IFR being less than 0.3% (i.e it is probably much higher).”
turns out things like vit d deficiency prolly doubles ur chances of dying.. i can get tge actual risk ratio. any way vit d deficiency is not uniform across populations. so…
not so sure about your lower bound.
the rate matters less i think than the rate given certain medical conditions..
Thanks Ben and Steven. Apart from it being a lot of dead people, it also happens pretty quickly, so it will have knock-on effects on others – plenty of other unavoidable deaths because hospitals are over-whelmed.
@Morpheus:
Apparently carefully explaining where the flaw in your argumentation lies is now slinging insults, whereas calling a group of respected scientists “a mob” is not. Strange times we live in.
“the IFR is probably bigger than 0.1%, but less than 1% (the kind of numbers I see popping up quite a lot are 0.3% to 0.4%). Do some disagree with this?”
Yes, 0.3 and 0.4% are not impossible, but extremely optimistic. I expect the value (when hospital care is good) to be between 0.5 and 1%. Like the meta-study of Joshua and Prof. Christan Drosten.
In Germany the Case Fatality Rate is 4.4%. https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-05-10-en.pdf?__blob=publicationFile
Mosher, is 3% still the CFR for South Korea?
So to get to an Infection Fatality Rate below 0.5, you would have to assume that only 1 in 10 infection is detected. That may be reasonable in America, but not in South Korea where testing and isolating is the main mitigation strategy. I would also be highly surprised if Germany only detects 10% of cases, while our testing is quite extensive; the positive test rate is on average 6.7%. https://de.wikipedia.org/wiki/COVID-19-Pandemie_in_Deutschland#Testkapazit%C3%A4ten_und_Anteil_positiver_Ergebnisse
Not quite sure why that’s a “Yes” 🙂 All I was getting at was that the evidence seems to be indicating that it probably isn’t than 0.1% and – I had thought – probably isn’t above 1% (although you seem to think that it may be in some cases).
Obviously you can’t really talk about the IFR in isolation from the context – pop age structure, strength of health system etc etc etc – but I think the best evidence tends to around 1.5%, in line with some of the orifgnal studdies out of China and elsewhere. See eg https://cmmid.github.io/topics/covid19/global_cfr_estimates.html
I also note that this is consistent with a country like Oz where the ascertaiment rate is almost certainly close to 1. Lots of testing from the start, growing in recent days, with positivity most cases are being detected. The current CFR is about 1.4% and unlikely to shift much from there, giving the very low new case and death rates. Similar story for NZ. In both places, the CFR is very likely close to the IFR.
Some text processing glitch in that last post, snipped: “… with positivity less than 1% overall and less than 0.1% recently. Minimal community spread cases popping up, implies most infections are being detected, traced and isolated.”
ATTP,
People want an answer and for the most part a politically convenient/expedient answer.
After the so-called real time facts, or the laying down of individuals confirmation biases, we will have the after-the-fact mortality data …
https://www.euromomo.eu/graphs-and-maps/
I also strongly disagree with this very naive idealistic comment of yours …
“However, that still doesn’t imply that we should simply pass on the responsibility to some unelected group; we should be doing things to reduce the influence of those donors and doing more to ensure that our elected leaders make decisions that are in our collective best interests.”
It IS primarily the so-called unelected that ARE misled by other MUCH MORE influential unelected that has gotten us to where we are yesterday, today and tomorrow.
Victor –
To the extent that Worldometers is comprehensive, the simple math there shows the CFR for Korea to be 2.3% (the simple math from Worldometers indeed returns 4.4% for Germany).
> So to get to an Infection Fatality Rate below 0.5, you would have to assume that only 1 in 10 infection is detected. That may be reasonable in America, but not in South Korea where testing and isolating is the main mitigation strategy. I would also be highly surprised if Germany only detects 10% of cases, while our testing is quite extensive; the positive test rate is on average 6.7%.
That one study estimated that the % positive for antibodies in Germany might be 1%-2%, so something like 800.000-1,600,000 Germans who are positive for the antibodies. Detecting 10% would mean between 80,000-166,000. Worldometers has 172,000 cases in Germany. So maybe we could ballpark the upper bound of the IFR in Germany at 0.44%? And I would imagine that the IFR would be lower in Germany than many other countries for a variety of reasons.
There, have I just proven that I fully deserved my advanced degree in armchair epidemiology?!?!
Anders –
> Can I clarify what the whole argument with DPY is about. From what I’ve seen, the fraction of people who’ve already been infected is probably less than 10% of the population, and the IFR is probably bigger than 0.1%, but less than 1% (the kind of numbers I see popping up quite a lot are 0.3% to 0.4%). Do some disagree with this?
IMO, the argument is about pretty much the same issue as any discussion with David – whether or not he’s able to acknowledge that he, like the people he criticizes, is influenced by his political biases when he looks at polities to address climate change of COVID-19.
As for “Do some disagree with this?” I kinda disagree with it, in that as SzAtWP01 speaks to above, (1) there’s really too much uncertainty to say at this point and, (2) “you can’t really talk about the IFR in isolation from the context”
My whole beef with David in this particular case is that he was defending Iaonnidis’ advocacy for broadly-applied policies based on extrapolating a national-level *fatality rate* from an *infection rate* calculated in a non-representative context using a non-random sample.
I’m still gob-smacked by that.
Sorry – for Germany that would be a lower bound….
Joshua,
Sure, I agree. The probably in my question was carrying quite a lot. Most of what I’ve seen to date is pointing to the IFR probably being below 1% in most cases. However, this will depend on other factors and we don’t know enough to yet determine this with much confidence.
Anders –
> Most of what I’ve seen to date is pointing to the IFR probably being below 1% in most cases. However, this will depend on other factors and we don’t know enough to yet determine this with much confidence.
Sure. But part of what is beneath the surface there is that he “most cases” includes an embedded difference whereby certain communities bear a disproportionate impact. I’m not saying that you’re doing that, but that it is something that is often not considered within the public discussion.
And then we have people like David – who flat out told me that the disproportionate impact in various communities is “irrelevant.” I kid you not.
https://judithcurry.com/2020/04/30/covid-discussion-thread-v/#comment-916343
Joshua,
Yes, I agree. A single IFR number hides a lot of detail about how different groups will be impacted in different ways.
> the disproportionate impact in various communities is “irrelevant.
Say the immunity wanes to zero in 12 months and there is no vaccine. Both are possible. How many die?
Say there are unknown knock-on-effects. As an example, say the chidden who experience a mild infection start dying of a viral infection when they are in their 50’s?
It’s a novel coronavirus, so Chinese doctors/medical scientists easily convinced their comparatively intelligent government officials to shut down a major part of their economy and lock up a significant portion of the population until the virus was essentially eradicated inside their country.
izen:
The primary purpose of democracy depends entirely on who you ask. Plutocrats usually get their way, but they don’t have carte blanche. Americans, at least, are complicit in our enfeeblement by the one percent. Their influence is tolerated by voters who value economic and social stability above all. We vote for the security of our families first and foremost, and hope some wealth trickles down to us. We’re willfully ignorant, too: we can look behind the curtain if we care to, but too few of us do. No conspiracy is airtight, after all: indeed, the modern concentration of power in the hands of the Koch club is documented in the public record. And we’re lazy: we want our “leaders” to make collective decisions for us, and not bother us with the fine print.
The fundamental problem with democracy is that those we’d trust most to wield power don’t seek it. Let’s not forget that plutocrats and politicians arise from among us. Who is surprised when they prioritize their self-interests? Yet those interests overlap, more or less, with our own. That means our political choices can only be on the margins. In every election, some
asscandidate is going to win. Which one do we distrust the least to act on our behalf?The primary purpose of the US Constitution’s framers wasn’t to ensure progressive government, but to forestall tyranny. They understood that no one who seeks power can be trusted with it. They also understood that all powerful persons have powerful enemies, making factionalism inevitable. So they built checks and balances into our founding document. Power seekers have to submit to popular acceptance repeatedly, beginning at the local level and working their way up, and the winners in each round have to cooperate to achieve their individual ends. Wealthy patronage helps, but doesn’t guarantee electoral victory: see my link above. Some basic rights for “ordinary” citizens are defined, including the right to know what our leaders are up to if we wish. A system of law courts provides citizens some protection from plutocratic whims, and allows access to the levers of power for anyone willing to make the effort. And while government claims a necessary monopoly on force, the Constitution brought us a country awash in guns, leaving open the option of armed rebellion or even civil war.
Of course the framers weren’t gods or even wizards, they were just guys. They managed to establish the rule of law pretty much as defined by the Constitution, but they knew it would always be precarious. And with some exceptions like Jefferson, they had no expectation of social progress; actually, it seems that for the sake of stability, they made “progress” as hard as possible. They left it to later generations of ordinary folks, with all our cognitive limitations, and just hoped we wouldn’t all be fooled all the time. IMHO they were more successful than history would predict. We all know things could be much worse. How bad they get from here, ultimately depends on our friends and neighbors. So vote blue! It’s a decision on the margin, regardless.
ATTP:
“Can I clarify what the whole argument with DPY is about. From what I’ve seen, the fraction of people who’ve already been infected is probably less than 10% of the population, and the IFR is probably bigger than 0.1%, but less than 1% (the kind of numbers I see popping up quite a lot are 0.3% to 0.4%). Do some disagree with this?”
Let’s not forget that the rate of transmission is also important. For an R0 of 3, you need about 66% of the population to become infected for herd immunity to kick in to the extent that it largely goes away. R0 for the most flus seem to hover around 1.5. For the 1918-19 pandemic, 1.8 (ignoring uncertainty intervals). Neil Ferguson used 1.8 for his modeling of a novel flu outbreak in Thailand (that’s what the model was originally built to do).
So a 0.1% IFR for covid-19’s going to kill more people than a 0.1% IFR for the flu, around twice as many people, actually, for the no intervention scenario. That’s important to remember since the focus on pushing the IFR down is to minimize the seriousness of covid-19.
And, of course, we do have tamiflu to protect health care workers. Ferguson’s model explicitly was looking into how many doses of tamiflu would be needed to be given to the general population to knock down a novel flu outbreak while still confined to Thailand for various levels of social isolation, number of cases when the outbreak was identified, etc.
Forgot the link to my source for estimated IFRs for various flus.
https://bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-14-480
Argh link is right but meant R0s not IFRs.
dhogaza,
Sure, I wasn’t trying to suggest that an IFR as low as 0.1% (which, from what I’ve seen, is probably too low) would imply that we don’t to implement any strategies to deal with this.
James Annan has an interesting post that tries to estimate the IFR from data from Guayas, Ecuador. Seems to get a best fit with an IFR of around 0.5%, but it could be higher. Makes the point that the population tends to be younger than in the UK, so this would suggest it’s lower than here, but the healthcare system was overwhelmed, which may have had an impact too.
OK. Now this is classic:
> Just 0.7% of Major League Baseball employees tested positive for antibodies to Covid-19. The small number of positive tests, came as the league continues to plan to start its delayed season.
[…]
“I was expecting a little bit of a higher number,” Bhattacharya said. “The set of people in the MLB employee population that we tested in some sense have been less affected by the Covid epidemic than their surrounding communities.”
——
So I expected a result based on my theory, and I tested my theory and got a different result. Obviously there must be something wrong with the sample I used because they didn’t March the results I expected.
https://www.google.com/amp/s/amp.theguardian.com/sport/2020/may/11/mlb-baseball-covid-19-coronavirus-antibodies-test
Also, please note (if you read the article) the researcher’s sudden focus in the media reports on the SES representativeness of the sample.
I mean in a sense that’s a good thing – but in the context of the PR campaign after the Santa Clara study, where they went on national TV to extrapolate from non-representative data, it’s pretty disturbing.
ATTP
“Sure, I wasn’t trying to suggest that an IFR as low as 0.1% (which, from what I’ve seen, is probably too low) would imply that we don’t to implement any strategies to deal with this.”
Oh, I didn’t think you are trying to suggest that …
ATTP
“Seems to get a best fit with an IFR of around 0.5%, but it could be higher”
He gets an equally good fit with an IFR of 0.4%. The question then is how effectively did that portion of Ecuador manage to lower Rt due to intervention. IFR 0.4% yields a post-intervention Rt of 0.94 which would be “hardly at all”. IFR of 1%, in his model, requires a post-intervention Rt of 0.5, which would be, as he points out , would be extremely good. So he suggests splitting the difference, 0.7%. With that figure the model fits well with an Rt of 0.58%, a bit less than his computed Rt for the UK.
I’ve been following someone who was in Ecuador until just recently (couldn’t get a flight to her home in NZ). She wasn’t in the same region but where she was, the lockdown was quite strictly enforced by the police.
Anyway, his range of IFRs are all in ballpark of what various other people are finding using various methodologies, excluding outliers favored by some.
And remember that WHO, back in February, sent a team into China and they concluded that the IFR is probably in the range of 0.3%-1%. Seems that’s held up quite well.
Steven –
Just saw the little turd you dropped for me here, and then saw the turd you dropped for me over at Judith’s. My response over there in case it doesn’t get through moderation (Judith gets very sensitive and protective about criticism of Nic).
—-
I’m not arguing arguing one way or the other.
What I’m saying is thst I can see people selecting comparison points, inevitably, to prove associations that agree with their ideological preferences.
I’ll give TE credit for at least bucking that trend. Nic, not so much. What it boils down to is the comprehensiveness of your treatment of the variables.
People are comparing to the economic effect of Sweden’s no lockdown policy without even attempting to control for the effect of the lockdowns in other countries as distinguished from the impact of a raging epidemic. They are making assumptions about the benefits economically to Sweden from no lockdown without even evaluating the economic state of Sweden. Your friend was comparing virus trends in Sweden and Switzerland a few weeks ago – not doing that now, is he? Why do you think he stopped? Maybe because he was making that comparison before enough time had passed to make the comparison meaningful.
“Skeptics” are often right when they raise questions about incontrolled variables. I have often said so.
It’s like when Nic tried to extrapolate from non-representative data on the Princess Diamond, and then had a double down by doing it too soon (missing a high percentage of deaths).
Above all, the question is really about consistency and evenly applied standards.
There are other rules that apply to appeals to uncertainty.
TE gets good marks on this issue in my opinion. He’s applying due skeptical diligence.
Extrapolating from unrepresentative data, trying to draw causal conclusions from cross-sectional (non longitudinal) data, and trying to infer causality from associations without presenting a plausible causal mechanism, get black marks in my book.
Selective treatment of uncertainty gets the biggest black mark.
Not even attempting to control for obvious variables, particularly ones that are quite likely explanatory, failing to do any kind of sensitivity analysis of similar variables, not addressing obvious potential confounds? Black mark, black mark, black mark, black mark, in my book.
The point isn’t to be perfect. The point isn’t to be correct. The point is to be transparent so that people can at least see that you’re trying to integrate the reality that you are the easiest person for you to fool. With that transparency you can be vulnerable and ask for help. It provides you that space to observe and breathe. You can be less reflexive. You can become detached.
ATTP: “Not quite sure why that’s a “Yes””
That was a “yes, I disagree that 0.3 to 0.4% is a good estimate”. Although technically you only claimed this was mentioned quite a lot.
My range of 0.5 to 1% is also partially chosen such as they are nice round numbers, thus not suggesting too much accuracy. I would be much less surprised if the scientific consensus in a year turns out to be above 1% than if it were below 0.5%.
Joshua: “That one study estimated that the % positive for antibodies in Germany might be 1%-2%, so something like 800.000-1,600,000 Germans who are positive for the antibodies.”
I am not sure which study you refer to.
In that range we have real problems with the accuracy of antibody tests, as you already mention above. One would have to do additional functional antibody tests, which is a lot of work, although fortunately the number of possibly positive samples will be small, and I have not seen any studies doing that. Later it will be easier as a larger percentage of the population has antibodies.
The alternative to having to do such extensive functional antibody testing is to test blood from people donating to blood banks. Then you can sample the same population multiple times. These people are likely not representative, take more care of their health, cannot donate if they were recently ill, but no estimate is perfect and having many different ways of doing it helps.
JCH: “Say the immunity wanes to zero in 12 months and there is no vaccine. Both are possible. How many die?”
Immunity is not a black and white matter. And when detecting antibodies is no longer possible, the immunity is not gone, especially in this case as other parts of the immune system do most of the heavy lifting.
We cannot be sure about anything over such a long time as the virus is new. But Drosten expects that as the virus is so widespread it will stay with us like to common cold, just like the other Corona viruses.
“Bhattacharya said the low number of positive tests showed there is a still long way to go in the pandemic. “It’s very clear,” Bhattacharya said, “that the epidemic is still in the early stages throughout the country.”
Victor –
This one:
https://medicalxpress.com/news/2020-05-team-covid-infection-fatality.html
As I recall they didn’t specify the basis for the Germany-wide infection rate speculation….
Willard – That’s funny.
“Mosher, is 3% still the CFR for South Korea?
https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030&act=view&list_no=367194&tag=&nPage=1
Victor.
10,909 confirmed cases
256 Dead.
another 41 in ICU waiting to be harvested
But
https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030&act=view&list_no=367188&tag=&nPage=1
see the age structure in the cases.
Short version: Early on a lot of the testing ( ~300K tests or so ) were focused on the churches
So a lot of younger people tested. tested positive and recovered.
The Other incidents of infection have been concentrated in group settings, nursing home,
hospitals, etc. and you end up with 25% of 80 year olds dying.
Looking at the data this much seems clear.
1. there is skew to the incidence and mortality by age
2. there is skew to the incidence and mortality by co morbidity.
3. there is skew to the mortality by gender
4. There is skew to the mortality by race
5. There is skew to incidence mortality by Vitamin d deficiency*
And dont even talk to me about the correlations between all those factors
so, I dont even want t talk about CFRs until I see actual mortality
data that is coded according to known factors that skew it.
basically I would want to see all the cross tabs.
Psst. protip
get yourself checked for Vit D deficiency. I had it years ago. A few shots and all fixed.
Do this irrespective of Covid. Here in Korea it is a standard shot every 90 days.
200000 IU, cost less than 30 bucks ( Asians apparently have a pre disposition to low Vit D)
I had no clue I had low Vit D . 42% of whites do. I sued to get horrible colds from all my travel.
no more. knock wood.
https://www.ncbi.nlm.nih.gov/pubmed/21310306
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3686844/
* https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3585561
https://www.technologynetworks.com/tn/news/researchers-have-discovered-a-strong-correlation-between-severe-vitamin-d-deficiency-and-mortality-334567
https://link.springer.com/article/10.1007/s40520-020-01570-8
When I look at Serology plans one thing I have looking for is do they do blood panels and report
on them. In other words are they learning anything about the profile of those who have the disease but never presented for diagnostic testing.
not finding much data
SM:
“Do this irrespective of Covid. Here in Korea it is a standard shot every 90 days.
200000 IU, cost less than 30 bucks ( Asians apparently have a pre disposition to low Vit D)”
Yeah, I’ve been doing 1000 units of D3 a day. Recommended by my doctor up north several years ago, when I moved the the Monterey area I stopped, not so much intentionally, more a result of the disorganization of my schedule and things when I moved. Started back up in March.
I haven’t had covid-19 since 🙂
ya dhog, when I moved to Norcal coast ( no sun, work inside) was when I first got hit with the
low Vit D. doc proscribed shots and prescription 10000 UI per day, . Now I just handle it with quarterly shots 200K UI
and better diet and 1000 UI per day.
Seems to me Cuomo ought to insure his non white population is tested. especially since they have to draw blood to do serology. he seems to like data
wack a mole in Seoul
This one’s better:
ATTP wrote on May 11, 2020 at 7:32 am:
“…the IFR is probably bigger than 0.1%, but less than 1% (the kind of numbers I see popping up quite a lot are 0.3% to 0.4%). Do some disagree with this?”
Yes, some disagree, at least especially with those numbers as low as 0.3% to 0.4%.
UW Researcher: COVID-19’s Infection-Fatality Rate 10 Times Larger Than Flu’s
https://www.managedhealthcareexecutive.com/news/uw-researcher-covid-19s-infection-fatality-rate-10-times-larger-flus
Quote:
“Assuming that 35.5 million Americans contract COVID-19, an assumption that is based on the number that contract seasonal flu, the researcher, Anirban Basu, says the 1.3% infection-fatality rate would mean nearly 500,000 COVID-19-related deaths in the U.S. this year.”
“To the extent that COVID-19 is more infectious than flu and does not have the protection from a vaccine or treatment, the number of deaths would be higher,” writes Basu, although he adds that “certainly with mitigation strategies, the death toll will be lower.””
And for the study:
Estimating The Infection Fatality Rate Among Symptomatic COVID-19 Cases In The United States.
https://www.ncbi.nlm.nih.gov/pubmed/32379502
From the abstract:
“Knowing the infection fatality rate (IFR) of SARS-CoV and SARS-CoV-2 infections is essential for the fight against the COVID-19 pandemic. Using data through April 20, 2020, we fit a statistical model to COVID-19 case fatality rates over time at the US county level to estimate the COVID-19 IFR among symptomatic cases (IFR-S) as time goes to infinity. The IFR-S in the US was estimated to be 1.3% (95% central credible interval: 0.6% to 2.1%). County-specific rates varied from 0.5% to 3.6%.”
It seems he did not use excess deaths beyond the “official” counts of who has died from Covid-19, and that he did not use the total count of all infected including asymptomatic cases. If this is the case, then this 1.3% IFR figure could be right as a *minimum* for what we could call a true natural IFR. (If the former changed, then the latter would have to change as well, and I emphasize “minimum” based on what I share below.)
This next article underscores what I shared in my prior post at May 11, 2020 at 7:00 am on the official death counts from Covid-19 being way too low, about what a true natural death rate might actually be:
Somali medics report rapid rise in deaths as Covid-19 fears grow
Concerns that official mortality counts in African countries are a big understatement
https://www.theguardian.com/world/2020/may/02/somali-medics-report-rapid-rise-in-deaths-as-covid-19-fears-grow
Quote:
“But evidence from medics and burial workers in Mogadishu, the capital of the unstable east African country, suggest the number of deaths could be many times higher.
Mohamed Osman Warsame, an ambulance driver, said he had transported between 15 and 18 corpses to cemeteries in the capital every day for the last two weeks, many times above the usual daily figure of between two and four.
“There are a lot of deaths. It is like we are in a deadly war. People are dying so fast,” Warsame said.”
People need to wake up that the official counts all over the world are pure BS. To reiterate, there is a massive cover-up going on with these “official” counts. So much of the world’s poor are in a “you’re entirely on your own, bub” situation, essentially no access to any medical intervention whatsoever, especially the world’s refugee population that are largely now in some developing countries with no meaningful access to even such basics as soap and clean water, much less access to other non-medical intervention such as proper nutrition and even just nutritional supplements.
To think about natural death rates and how high they could be, and what it means, for comparisons, consider the fact that Native Americans had never experienced such as smallpox, measles, or flu before the Europeans came, and the viruses tore through these native populations, killing an estimated 90% of them.
Some final points, since Steven Mosher mentioned Vitamin D on May 12, 2020 at 2:42 am, and I mentioned nutrition above, here are two links I saw last week, one a lay abstract, the other a formal one, on a study covering some of Europe:
The role of Vitamin D in the prevention of Coronavirus Disease 2019 infection and mortality
https://www.researchsquare.com/article/rs-21211/v1
https://www.ncbi.nlm.nih.gov/pubmed/32377965
And here is something on Vitamin K, believe it or not:
Reduced Vitamin K Status as A Potentially Modifiable Prognostic Risk Factor in COVID-19
https://www.preprints.org/manuscript/202004.0457/v1
From the abstract:
“Results: Dp-ucMGP levels were significantly elevated in COVID-19 patients (1,673A}1,584 pmol/L) compared to controls (536?291 pmol/L; p<0.0005). Dp-ucMGP levels were significantly higher in COVID-19 patients with unfavorable outcome compared to those with less severe disease. Furthermore, dp-ucMGP and desmosine levels were significantly associated (r=0.65; p<0.0005). Conclusions: Vitamin K status was reduced in patients with COVID-19 and related to poor prognosis. Also, low vitamin K status seems to be associated with accelerated elastin degradation. An intervention trial is now needed to assess whether vitamin K administration improves outcome in patients with COVID-19."
Very important: These dp-ucMGP levels are inversely related to Vitamin K status, the higher the dp-ucMGP, the lower the Vitamin K status, and the converse. There is an article I did not link to in which the journalist commits a typo in which it puts forth the idea that the higher the dp-ucMGP, the higher the Vitamin K status. So do not be confused by that – go with what the abstract of the study says.
This is provocative since Vitamin K promotes healthy clotting and we are starting to find out that clotting is what is killing some people, in that micro-clotting in the blood vessels in the lungs interfere enough with oxygen transport so as to cause people to suffocate to death. And what is scary is that according to some of what I've read, sometimes even high doses of some blood thinners do not work, do not stop this clotting problem.
Researchers try to solve the mystery of COVID-19 'storm of blood clots'
https://www.sfgate.com/science/article/COVID-19-blood-clots-deadly-15262756.php
Quote:
"Some clots are pudding-like globs of cells and proteins that can cause strokes when they reach the brain. Others are so tiny they can clog up capillaries. Blood thinners don't seem to work."
Other articles say that blood thinners are helping some. But which ones are used is important because some (many of the older ones) are Vitamin K antagonists (which means they drive down Vitamin K status significantly) and some (many of the newer ones) are not, and evidently Vitamin K status is important as well, based on the above study, to see how Vitamin K status relates to which blood thinners work and when blood thinners work.
But here is how this Vitamin K study above could help to make sense of all this: It seems that one of the functions of Vitamin K that almost everyone might not know about is that it works to regulate clotting, in that it works to prevent runaway clotting or clotting spinning out of control, which is what this virus seems to want to do. If it really is true that this is one of the evidently many functions of at least some of the many different forms of Vitamin K (K1, and the many menaquinone forms of K2), it could be very relevant to answering all these questions.
Or this related study on Vitamin K (one of the authors was involved in both studies) could help to make sense of all this:
Low Vitamin K Status Is Associated with Increased Elastin Degradation in Chronic Obstructive Pulmonary Disease
https://www.ncbi.nlm.nih.gov/pubmed/31357639
It might be unwise to focus on specific vitamin levels having a direct influence on the progression of COVID19.
The way our health is related to diet has less to do with the specific levels of individual components rather than the overall balance and diversity of what is, and isn’t, consumed. In that sense it is more like an ecology, the prevalence of a particular chemicals (species?) may be an indicator of the overall resilience and stability of the totality, but that does not mean it is a causative or primary determinative factor.
And then there is the added complication that this ‘ecology’ of a diet inhabits very diverse environmental ‘niches’ in terms of the specific genetic and developmental contingencies of the individual consuming it.
Short of total absence or extreme excess of certain components, the correlation between vitamin levels and health outcomes probably indicates more about the problems with the totality of what is consumed rather than specific shortages that can be easily corrected with a pill or shot.
Blue – OC43 – Human coronavirus (HCoV-OC43)
Red – HKU1 – Human coronavirus (HCoV-HKU1)
Black – SARS-CoV-2
Willard –
Funnier still:
> Andrew says:
May 12, 2020 at 8:11 am
David:
When people point out false or misleading things you’ve said, it’s inappropriate to give them “the bronze medal for nit picking.” This is a statistics blog. Details matter, and if you don’t care about details, you’re kinda wasting our time here.
If people go to the trouble of carefully reading what you’ve written and they find untrue or misleading statements, you should thank them for their effort, not criticize them for “nit picking.” If you can’t appreciate when people correct you, you should avoid open discussion forums like this blog. It would make more sense for you to be giving Ted talks or writing articles for PNAS or Perspectives on Psychological Science.
https://statmodeling.stat.columbia.edu/2020/05/08/so-the-real-scandal-is-why-did-anyone-ever-listen-to-this-guy/#comment-1335401
Gawd it is astounding who gets Palmer and Stevens butt backwards.
JCH –
He’s been selectively quote-mining their work for months.
Joshua,
I see Andrew Gelman is also discovering the joy of having DY commenting on his blog.
Anders –
I assume you saw the James Annan variation on the theme?
Joshua
“He’s been selectively quote-mining their work for months.”
I should’ve known that the Palmer and Stevens schtick wasn’t new. Oh, well, he got me to read an interesting paper.
Andrew’s comment was a coffee-splurfingly funny way to start the day …
Andrew says:
May 11, 2020 at 10:06 pm
David:
I recommend avoiding statements such as, “Every honest scientist already knew this.” Lots of scientists are ignorant of all sorts of things. That doesn’t mean they’re dishonest.
….
“David Young says:
May 12, 2020 at 9:37 am
Well Andrew, …
…
What surprises me is that you allow people to throw around ad hominems like “a pattern of deliberate deception.” This Is untrue and needs to be corrected.
….
plus ca change, plus c’est la meme chose…
Joshua,
I saw DY had commented on one of James’s posts. Is that what you’re referring to?
Anders –
The one where he gave David the opportunity to be accountable (didn’t work out so well) – I see that you commented, I had forgotten about that.
http://julesandjames.blogspot.com/2020/04/euromomo_10.html?m=1
BTW – Do you know why James has two blogs? I assume some sort of category distinction.
Joshua,
I think the one you link to above is the one they’ve been using for a long time. The new one they started (I think) when they returned from Japan and started their research company. It’s intended, I think, to be a bit more formal and James has been posting some of the more formal analyses on the new blog, rather than on the old one.
Well, this comment aged well:
Not sure about the second part, but I still like it.
> David Young will no doubt come flying in on his pig and agree that Nic’s analyses aren’t generally to be trusted
A basic misunderstanding on James’ part.
That would never happen., James’ scenario would require actually considering the specifics of Nic’s analystical process, rather than just responding to the valence of Nic as an ideological advocate.
Steven –
This is the kind of discussion I prefer over facile comparisons without controlling for variables and considering confounds. It helps to explain why you are misunderstanding me if you think I’m just making a simplistic appeal to uncertainty:
> (3) Concerning Sweden, Die Welt (in German) looks at what it calls the Swedish Sonderweg (“special road [taken or followed]”). Notably, it does not attribute the much higher mortality (compared to fellow Scandinavian countries) just to its not entering a lockdown (some voluntary social distancing measures are in place) — but to the “limping” Swedish healthcare system (marodes Gesundheitssystem).
They are at pains to point out that this is not a matter of money — Sweden has the 2nd highest pro capita spending in the EU, after Germany — but of inefficiency, administrative bloat, and wastage. Once upon a time, Sweden had 49.5 ICU beds per 100,000 inhabitants, which today would be the highest in the world, above even the USA. Today? Just 5.8.
Even before the COVID19 crisis, 12% of elective surgery patients has to wait 4 months or more, compared to 2% in France and none at all in Germany. One-fifth of Swedes have to wait more than 2 months for a specialist appointment, compared to only 3% in Germany.
Much like Israel’s public system, rapid access for life-threatening emergencies in Sweden is maintained at the expense of ever greater delays for everything else. [But much unlike Israel, Sweden entered the present crisis without the benefit of a young population and a warm, sunny winter and spring climate…] Doctors in the public system are salaried employees of the state, with all that entails in terms of (lack of) incentives…
“Some final points, since Steven Mosher mentioned Vitamin D on May 12, 2020 at 2:42 am,”
just to clarify somewhat. If you have a vitamin d DEFICIENCY ( as I did in the past) then you should fix it regardless. I’m not a doctor so check with yours.
Good news, everyone:
https://statmodeling.stat.columbia.edu/2020/05/08/so-the-real-scandal-is-why-did-anyone-ever-listen-to-this-guy/#comment-1335522
It’s just a flesh wound.
Joshua:
Wow. DY tried to peddle his comically inept spin of Palmer and Stevens on RC last year. Apparently the thorough fisking he got from multiple climate realists at the time, didn’t deter him from rebunking it elsewhere. OTOH, he hasn’t been back to comment on RC since…
James Annan:
Splutter 8^D! I’m not cashing out my 401k, in a down market, to buy stock in large, sturdy umbrellas!
Joshua: “Concerning Sweden, Die Welt (in German) looks at what it calls the Swedish Sonderweg (“special road [taken or followed]”).”
The German word “Sonderweg” is full of meaning. Before WWII conservatives used it as a positive term, a bit like American exceptionalism. Nowadays it signifies the failed historical path to modernization that resulted in the second world war and the destruction of Germany. “Sonder” sounds like weird, deviant and isolated.
The author is expressing that the route Sweden goes is isolated and leads to death and ruin.
180 degrees different from the “opinion” expressed in UK newspapers, Germany does whatever it can to stay away from the Sounderweg to ruin. That is the lesson learned from WWII. That is why Germany does not want to lead Europe, even if it is hard to avoid as the biggest country. It prefers to coordinate in the background, to join coalitions, to support the candidates of other countries. If you want to convince a German to do something, you need to tell them that everyone else does it. They do not ever want to go at it alone again, to press ahead, to see everything turn into rubble.
I presume the enormous enthusiasm of America for war is because America has never experienced a modern war on its own territory.
man this gets dicey
Ok. There is an outbreak in Seoul. It started in the gay clubs.
When the people who reported for tested were interviewed one young man says
he has no job.
So they track his movements.
he was a school instructure.
5 of his students tested positive
https://en.yna.co.kr/view/AEN20200513005000315
There is a moral in here somewhere.
On May 12, 2020 at 12:36 pm, izen wrote:
“The way our health is related to diet has less to do with the specific levels of individual components rather than the overall balance and diversity of what is, and isn’t, consumed.”
Yes, I strongly agree hat balance is important, and diversity, and at the same time, these studies I share are not about just balance, but about the fact that we are what we eat even in terms of individual nutrients, and they have effects, good and bad, as I will show shortly as to what some studies have found on certain different forms of Vitamin E, as an example that has been shocking to me since it was so unexpected and could be very important in relation to Covid-19, in that it could help even save lives depending on what people do in response to this info.
As to why I am sharing all this nutritional info, I am care-taking my 96 year old father and 89 year old mother and yes, am very worried about this virus, and so I am taking very seriously all the studies out there in the aggregate and assume that some of whomever might read what I write might be happy to know this info. And in light of that:
Several weeks ago I discovered that the two different different forms of Vitamin E called alpha tocopherol and gamma tocopherol have opposite effects with respect to lung inflammation, alpha tocopherol decreases it, and gamma tocopherol actually increases it. (There are four tocopherols and four tocotrienols.) I found this shocking since so many Vitamin E supplements out there promote gamma tocopherol, and so in addition to eating oils high in gamma tocopherol and especially taking the very high amounts of gamma tocopherol in these pills might be the worse thing we can do to prepare ourselves for this virus, which goes straight for the lungs.
Needless to say, several weeks ago I changed our diets and supplement regimens to account for this as well as everything else I’ve found.
Google
gamma tocopherol lung inflammation
and be prepared to be shocked. In the US the average plasma gamma tocopherol is high due to high consumption of soybean, corn, and canola oils, which are high in gamma tocopherol. Some sources say that these levels roughly average about four times higher than they are in many European countries that, instead of using the mentioned oils in their diets, use such as sunflower or olive oils, which are are very low in gamma tocopherol. (Very unfortunately, gamma tocopherol is high in many popular high fat foods (and of course the oils from them) beyond what I mentioned, such as flaxseed (linseed), pecans, pistachios, pine nuts, walnuts, cottonseed, palm, sesame seeds, and pumpkin seeds, Some of the high fat foods and their oils very low in gamma tocopherol beyond the ones I mentioned are coconuts, avacado, safflower, almonds, macadamias, hazelnuts, and grapeseed. But peanuts, Brazilnuts, poppy seeds, and cashews are moderately high, but still quite high compared to the ones I said are very low. Charts can be found all over.
Here are some of the many studies and articles about studies out there – the one immediately below is a human study that followed the animal studies of which I sample further below:
Vitamin E in canola, other oils hurts lungs
https://www.sciencedaily.com/releases/2014/05/140520220424.htm
Quotes:
“The new study shows drastically different health effects of vitamin E depending on its form. The form of Vitamin E called gamma-tocopherol in the ubiquitous soybean, corn and canola oils is associated with decreased lung function in humans, the study reports. The other form of Vitamin E, alpha-tocopherol, which is found in olive and sunflower oils, does the opposite. It associated with better lung function.
..
This is the first study to show gamma-tocopherol is associated with worse lung function.
..
She found that a high level of gamma-tocoperol, 10 micromolar in the blood plasma, was associated with a 10 to 17 percent reduction in lung function.
…
Here is the study:
The vitamin E isoforms alpha-tocopherol and gamma-tocopherol have opposite associations with spirometric parameters: the CARDIA study
https://respiratory-research.biomedcentral.com/track/pdf/10.1186/1465-9921-15-31
This above study followed such studies as the following:
Two Faces of Vitamin E in the Lung
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3778733/
Quotes:
“The marked rise in rates of asthma over a few decades and the differences in rates among countries and in migrating populations suggest an important role of the local environment, such as diet, in development of asthma. One environmental change over the past 40 years has been an increase in the gamma-tocopherol isoform of vitamin E in the diet and in infant formulas. We recently demonstrated that gamma-tocopherol increases allergic lung inflammation in mice (6-8).
..
We have additionally demonstrated opposing regulatory functions of alpha-tocopherol and gamma-tocopherol in mice and the mechanisms for anti- and proinflammatory functions of these tocopherols (7, 8, 28, 30, 31).
…
In the United States, the average human plasma gamma-tocopherol levels are two to five times higher than those of many European and Asian countries (Figure 1B), whereas the average human plasma alpha-tocopherol levels are relatively similar among these countries (28). This fivefold higher level of human plasma gamma-tocopherol is similar to the fivefold increase in plasma gamma-tocopherol in mice that increased allergic lung inflammation with gamma-tocopherol administration (8). The high human plasma gamma-tocopherol levels in the United States are consistent with soybean oil, which is high in gamma-tocopherol (53, 54) (Figure 1C), as the predominant food oil in the United States (55, 56).
One of the studies I don’t link to here showed that high doses of alpha tocopherol reverses the problems caused by gamma tocopherol, but only if gamma tocopherol was not in the mix such as in mixed tocopherols that can also be present in these supplements and such as in any base oil not being one of those I mentioned being high or moderately high in gamma tocopherol. I calculated from that study the human equivalent of 600 IU per day, well below the UL (the safe upper limit) here in the US of 1000 IU per day.
However, it turns out that high doses of alpha tocopherol very significantly drive down levels of Vitamin K, which would be a very bad in light of what I shared in my previous post on May 12, 2020 at 9:20 am with a study linking higher Vitamin K status to better Covid-19 outcomes and the converse.
Side note: (What I say next holds regardless of the d- or dl- forms of E, but I?d stick with the natural d- forms.) In one study, even high doses of alpha tocopherol succinate did not do much at all in terms of raising plasma levels of alpha tocopherol, and so the purported anti-cancer effects of alpha tocopherol succinate in some studies are evidently based on the form not breaking down. This is different than the alpha tocopherol acetate form, which does break down so as to significantly raise plasma alpha tocopherol. But since this acetate form is a synthetic hybrid, I’d stay away from it, since it is linked to higher rates of cancer and other problems such as what we here about vaping products destroying the lungs, where some think the acetate is what is messing up the lungs. Stick to the pure d-alpha tocopherol form, no acetate forms, but if the succinate form is taken, also take the straight alpha tocopherol form to get the plasma alpha tocopherol up.
Getting back to my point, if we are going to take supplemental Vitamin E, then we really need to take supplemental Vitamin K as well, K1 and the MK-7 form of K2.
Here is some information on all this, a study that shows that 1000 IU of alpha tocopherol per day significantly drives down Vitamin K status (but from what I’ve read, it seems that it’s been known for decades that high intakes of alpha tocopherol can drive down Vitamin K status):
Effect of vitamin E supplementation on vitamin K status in adults with normal coagulation status.
https://www.ncbi.nlm.nih.gov/pubmed/15213041
If you enjoy ‘facile comparisons’, looking at the difference between Argentina and Brazil is interesting.
Brazil has a big population, so if things continue to go badly there, it may end up being the worst-hit in terms of absolute numbers.
Check in procedure at seoul airport fastidious. 3 different temp checks. Flight has 10 people or so.
Safe travels boys
Boy, that escalated quickly:
Willard, you’ve been had. That’s clearly a parody account.
I assumed that would embed. Can you sort it, O wise and benevolent moderators?
[Mod: Sorted. Seems to not embed if it’s the mobile version.]
Great article, IMO, for reflecting on the COVID-19/Climate change parallels. Absolutely perfect that Raoult is a “skeptic.”
Alan is a regular at the ClimateBall honey trap, Very Tall, e.g.:
In other news:
https://www.nature.com/articles/s41586-020-2281-1
And then there’s the Contrarian Matrix.
I’m posting the following for “a friend” who has some questions about the following and was looking for feedback:
> The point of that post was that the biggest example of this confusion is the climate sensitivity. A more precise estimate is said to be worth $10 trillion dollars but the spread around the central value has changed little in decades. That is actually because what they are calling “uncertainty” is a descriptive statistic that will not decrease in response to more data:
It seems sigma_f is simply the residual standard error of this linear regression. This is a property of the linear fit and data, it will not become more precise by collecting more data (unless the relationship between temp anomaly and forcing becomes more linear). In other words, the range of values for climate sensitivity is a derived property of the data (plus assuming a linear relationship between temp and forcing). It is not supposed to get more precise any more than standard deviation is supposed to approach zero as you collect more data. The priors are supposed to be used on f and sigma_f, not on climate sensitivity.
https://statmodeling.stat.columbia.edu/2015/12/10/28302/#comment-254706
Basically, the climate sensitivity to CO2 is not a constant. The effect of CO2 varies depending on what is going on with the rest of the Earth/Sun system. This variation is not an uncertainty that decreases as more data is collected.
+++++++++++++++++++++++++++++++++++++++++
Might be a little hard to follow out of context (not sure what context I could provide) but I told my friend that I’d be happy to post the comment here to see if anyone bites. If anyone does want to bite they could respond here and I’ll relay the response, or at the link where my friend left the comment:
https://statmodeling.stat.columbia.edu/2020/05/10/uncertainty-and-variation-as-distinct-concepts/#comment-1334183
Joshua,
I don’t think it’s correct that we don’t expect estimates for climate sensitivity to get more precise. There will be some inherent variability, which means we won’t settle to a very precise temperature if/when we double atmospheric CO2. However, this is not going to be large enough for the temperature to vary from 1.5C to 4.5C (i.e., if/when we double atmospheric CO2, we’ll clearly have a more precise understanding of cimate sensitivity). We could also average over some time interval, which would then average out some of this inherent variability.
Willard
Here’s the link to the government report. Moncloa is the national government complex in Madrid.
https://www.lamoncloa.gob.es/serviciosdeprensa/notasprensa/sanidad14/Paginas/2020/130520-seroprevalencia.aspx
Can anybody name a lethal virus to which the human population of the earth has achieved herd immunity without a vaccine? Even with vaccines, some viruses do quite well.
Some relatively old news on the French front:
https://www.medrxiv.org/content/10.1101/2020.04.18.20071134v1
Asymptomatic transmission model:
https://medicalxpress.com/news/2020-05-covid-silent-explores-role-symptomless.html
Vit D
But what on earth are they talking about? Name a virus to which the humans of the earth have achieved herd immunity? Small Pox? Rabies!! HIV? Measles? Mumps? Seasonal flu? Human coronaviruses? Chickenpox? It only happens when there is a vaccine.
May be a reason why they call it herd immunity rather than population immunity.
Some diseases gone:
https://en.m.wikipedia.org/wiki/Eradication_of_infectious_diseases
Personally i would not put too much trust in people of power who view you as a “herd”
But thats just me
ATTP wrote “I don’t think it’s correct that we don’t expect estimates for climate sensitivity to get more precise. ”
Unless we discover more “unknown unknowns” Turning an unknown unknown into a known unknown is real scientific progress, but it will tend to broaden the range of plausible climate sensitivity rather than narrow it. I expect they will become somewhat more precise with time, but not uniformly so, and probably not very quickly. That doesn’t mean we have learned nothing about CS since e.g. the Charney report, quite the opposite, though many skeptics would like to argue otherwise! ;o)
Dikran,
My point is that I think the 1.5C – 4.5C mostly represents our uncertainties in the physical processes, rather than representing some real physical range. In other words, if we were able to run the world many times and double atmospheric CO2 from the same initial state, it would tend towards a well-defined climate sensitivity. It wouldn’t end up with 66% of the final states lying inside 1.5C – 4.5C and 34% ending up outside that range.
ATTP, yes, I agree that is the likely cause of most of the spread, but I think the “unknown unknowns” part has also been a non-negligible component. ISTR some climate scientist mentioning that, but I can’t remember who and can’t find the quote.
It is essentially a [subjectivist?] Bayesian sort of uncertainty rather than a frequentist one.
Dikran,
Sure, but I don’t think the unknown unknowns implies that the range is somehow physically real. It might end up being higher, or lower, than we expect, but it’s probably still – essentially – a well-defined value (I think).
ATTP, is one way of looking at it that we’re essentially living in one world which corresponds to one realisation of a perfect, idealised GCM? Even with perfect physics initialised with perfect* data, we’d expect some variation in the final outcome. When we eventually get there, we’ll know we’re in realisation 172397 and not 625154, but not before. There’s no reason why our iteration should be the P50 of all possible iterations. That doesn’t mean that the ECS we’re carrying today was “wrong”.
Presumably as we get closer the range will narrow because, as the latitudinally sectored ECS estimates showed, which parts are heating more and which parts are getting more or less cloudy matters. As time goes on we can expect to lock in modes of climate such as strong or weak AMOC, strong or weak polar amplification, ENSO state favoured one way or another, high cloud vs. low cloud, effective loss of Arctic sea ice during a freak summer which can’t be recovered, etc., which will lock us out of some end-states because it will take an extremely large perturbation (a very large volcanic eruption, perhaps) to kick us back onto that path. IOW the system does have some long-term memory of previous states, the most extreme of which is a bifurcation.
Of course we don’t have perfect physics or perfect data, so as well as path selection effects we can presumably expect ranges to narrow as we gather more data spatially, as time series get longer, as faster computers allow us to model explicitly rather then upscale, etc. But that mostly applies to model-based estimates. Ones using analogous past eras have structural uncertainties which won’t go away, such as uncertainties about ocean chemistry and about evolutionary adaptation changing some of the proxies. We see that with one of the planktonic proxies: the proportion of thick-vs. thin-shelled organisms changes between warm and cool periods, and there are subtle differences between them in their isotopic response to temperature. That’s one reason why it’s easier to say “this event warmed by 4°C” than to say “it warmed from 6°C above pre-industrial to 10°C above pre-industrial”.
* You might say that with some of the components chaotic, there’s no such thing as perfect data. You can get very close, but the outcomes will diverge over time.
The point about the role of parametric and statistical uncertainty vs epistemic uncertainty (unknown unknowns) is an important one. Really you want to improve model skill rather than just reduce the estimated uncertainty of the predictions.
I guess it would be nice to quantify this in a post-hoc way: once you have added a bunch of additional physics to, say, a climate model, randomly turn various terms off and see how much error it introduces. Do model predictions follow a random walk in time as more physics gets added?
James Annan was making some points about trying to understand how to interpret multi-model ensembles of climate simulations: i.e. does any point in the cloud represent a plausible prediction, or are these ‘independent measurements’ so the true answer is likely to lie much closer to the mean?
Ben,
Yes, James has a post about the truth-centered paradigm, which I largely agree with.
“Sure, but I don’t think the unknown unknowns implies that the range is somehow physically real”
Yes, it is “epistemic” rather than “aleatory” uncertainty?
The truth-centered paradigm can’t be correct “The ensemble mean is an estimate of the forced climate change, and the observations are (as I understand it) the combination of the forced and unforced change, so there is no reason to expect the observations to lie close to the ensemble mean, even is the the “standard” paradigm were valid. ”
If we had a set of parallel Earths that only varied in their initial conditions, then the “truth centered paradigm” would only be valid if our particular Earth happened to exactly coincide with the average of all the parallel Earths. There is no good reason to expect that to be the case. As James points out, it is closer to being true for things that involve a lot of spatial or temporal averaging, but even for CS wouldn’t expect the *observed* CS to be identical on all of the parallel Earths either.
This is a good way of putting it
Yes, we know that internal variability can influence the path, but probably doesn’t much influence the mean of the final state.
While aleatory uncertainty may be expected to averaged out in some cases to give a “truth-centered” paradigm, I don’t see any reason to expect that to be true of epistemic uncertainty (i.e. that our hypotheses about the climate a unbiased in a statistical sense).
I think it is easy to confuse CS as a “population parameter” which is determined by physics and a sample estimate of CS (or even a single observation of CS) which has some aleatory uncertainty. If you take one climate model with fixed parameters and estimate the CS from each run, you’ll get a slightly different value each time Taking the average of this will give us the sample mean, but that is not the same as the population mean which is determined by the code in the climate model. The population CS would be the mean CS over an infinite sample. This is also different from observed CS, which would be like the CS estimated from one particular model run.
If we were confident that the model physics were sufficiently correct [as we don’t actually have access to parallel Earths], we might be able to use this as a means of partitioning the total uncertainty into its epistemic (uncertainty in parameter values) and its aleatory (variation between runs) components. I think it would tell us that the aleatory uncertainty is fairly minor.
Dikran,
I guess I’m thinking of a hypothetical scenario where we consider an actual Earth with the same initial external conditions, but different initial internal conditions. If the only change were that we were then to double atmospheric CO2, then we would (I think) expect them all to converge towards the same mean final state (i.e., we wouldn’t expect the final states to reflect our current uncertainty in climate sensitivity). I’m still thinking in terms of the comment that Joshua posted, which seemed to be suggesting that the climate sensitivity range is somehow a reflection of the real system, rather than mostly being a reflection of our uncertainty about the underlying physical processes (I hope I’ve expressed that clearly).
I think it would in a very idealised setting, e.g. with a very long observation period (much longer than the longest mode of internal variability), but I’m probably being too practical in my thinking where that period may be unrealistically long. I’m not sure how long that period would need to be – centuries at least?
It certainly isn’t an uncertainty of the real system though, I fully agree there. “Weather” properties, e.g. decadal trends, are dominated by aleatory uncertainty, but not climatological properties such as CS.
Dikran,
Yes, I don’t think we’re going to narrow the uncertainty any time soon.
Ah, I see a flurry of parallel comments about parallel Earths 😉
Part of my point was as per dikran’s: there’s no reason why our particular pathway should correspond to the mean of all possible pathways for the same perfect climate simulation. Even if conservation of energy means that eventually all pathways converge to something similar for a given forcing (say, 2 x CO2e), if “eventually” means 500 years we care about which divergent pathway we’re on in the meantime. And at least conceptually, I can envisage albedo bifurcations such as a cloudy Earth vs. a partially cloudy Earth which cause two pathways to diverge irreversibly.
It’s an area which could be (possibly is?) being looked at. One of the the criticisms of LC18 is that sectored energy-balance models give a different ECS for the same dataset. And there is some understanding of which feedbacks and other causes are responsible. The Earth is currently in a mode where average global surface warming is less than the mean of the range of outcomes for the sectored ECS. An argument for using the mean and not our realisation is that in 50 or 100 years time we may lie equally far to the other side.
But you could play devil’s advocate and ask at which point we have enough information about the climate in our iteration of Planet Earth to say that some theoretically possible pathways can no longer be part of our future, because of the particular pathway we’re on for better or for worse. IOW if our future is constrained to a set of pathways which span only the P30 to the P95, we should consider the mean outcome of only those pathways when projecting an average future. One way to look at that would be to see whether many, few or no iterations wander from well on the hot side of the mean to well on the cold side, and over what sort of timeframe. Since it would be trivial to write a script to test that on an ensemble of outcomes I suspect it’s been done, if only out of curiosity. Another, which is being done although perhaps not for that specific purpose, is to screen models and realisations for those which best match structural aspects of our actual iteration, such as cloudiness during a particular ENSO phase, polar amplification or high vs. low cloud.
Dave_Geologist:
The discussion of the sources of model uncertainty is very interesting. IIUC, D_G’s point is about the narrowing of potential scenarios for forcing over time. This brings us back to the “RCPs are predictions” brouhaha, no? For a given RCP, a GCM outputs CS as a PDF accounting for internal, i.e. unforced variables. It’s external forcing that varies by RCP. Exactly which RCP represents the particular pathway we’re actually on, won’t be known until we reach an equilibrium climate. Is DM’s “epistemic” uncertainty mainly about which RCP turns out to be the real one?
> This brings us back to the “RCPs are predictions” brouhaha, no?
More generally, this brings us to the idea that models are supposed to guide action but can’t replace common sense.
My own heuristic does not follow graphs, it’s based on my competitive experience. When facing a very powerful enemy, it makes sense to shut down the position completely, as it neutralizes the edge the enemy has. You can’t just stay there, you need to “get out” of your shell and do something, it’s risky but the alternative is worse.
But a clamped position can’t be opened up all of a sudden, you get crushed by the opponent dynamic play; so you manoeuver, and release pressure by increment, ideally you simplify. At no point are your moves dictated by sudden panic – it’s just common sense after you lost a few dozens of games by failing to follow these principles.
Under that light, the argument is quite simple:
1. a lockdown was needed, at least it made sense as there was no alternative and the idea is sound
2. a lockdown carries a cost, we can’t live under siege for long, more so that vaccines are too far away and we don’t even know if there won’t be another iteration of the infection
3. we need to release the constraints, but not so fast as to lose control of the situation.
None of that requires projections of IFR or what not.
Same with climate, really.
Willard –
> 2. a lockdown carries a cost…
Sure – but I’ll go to my standard cost vs. price and externalities question – although no one else seems to be very interested in that and most people seem to virtually role their eyes when I reaise it.
> I’ll go to my standard cost vs. price and externalities question
The reason you ask that question is because you don’t have the answer, Joshua.
Contrarians use that trick all the time. Stop using it.
Willard –
> The reason you ask that question is because you don’t have the answer, Joshua.
The reason I ask that question is because I think it’s important to consider.
> Contrarians use that trick all the time. Stop using it.
Steven also seem to be accusing me of appealing to uncertainty. You’re both wrong, but you’re both entitled to be wrong.
> The reason I ask that question is because I think it’s important to consider.
Hence why you never answer it.
My point is that I don’t need to answer that kind of question. Yet here you are, burdening me with it.
Fancy that.
Willard –
> My point is that I don’t need to answer that kind of question. Yet here you are, burdening me with it.
Of course you don’t need to answer it, and I”m not burdening you with anything. You are entirely entitled to address it or not. Completely up to you. Obviously. Also, it’s up to you whether or not you feel burdened by it.
> I”m not burdening you with anything.
Of course not:
Tell me how externalities will help anyone make a decision in the following case:
https://twitter.com/nevaudit/status/1260955364318642177
Willard –
Why are you burdening me with a question you didn’t answer?
See where that goes?
> Why are you burdening me with a question you didn’t answer?
I already provided my answer, dear Joshua:
After playing Socrates you’re now pulling a variation on what we usually call Plato’s beard. So right. You bet I know where we’re going.
I will also clarify something else. All my previous sentences have been made of my own volition. I hereby declare I was free to make them. I also freely declare that my liberty to state them does not refute the reality of pragmatic commitments.
On a related note:
Jesus Willard, tell me that isn’t true.
It’s like they never read the history of SARS deaths in HK and the importance of ventilation testing in facilities
Another coming problem.
Power tests for vaccine trials.
The way an effectiveness test is done is volunteers are innoculated and then you wait.
you wait for them to randomly encounter the virus and mount a defense against it.
what is the problem? attack rate. if the attack rate is low ( like 1% ) and you are looking for
a 50% effectiveness, you need 10,000 volunteers.
in a CHALLENGE test, you dose the volunteer and expose them directly to the virus.
people dont want to do that for moral reasons. They dont want to infect the person on purpose,
they will let it happen by chance (see the trolley problem)
instead you will have.
A) A public you ere encouraging to protect themselves (masks, social distance, hygiene)
B) a set of volunteers you send out to see if they get infected by chance… by not
practicing these measures.
That’s a weird little moral distinction in there.
in any case, if you have too few volunteers they will never be exposed to the virus, or
exposed to different strains, or exposed, but innate immunity will kick in and there will be
antibody response.
there are 90 vaccines in the pipeline.. it is easy to see more than 1 million volunteers needed in total, some are planning for 30-40K at huge expense.
Meanwhile –
W/r/t Ioannidis’ “just like the flu” (paraphrasing), and David’s truncating the likely range of the IFR estimates….
They say 0.1 for the flu, right? (with vaccines, obviously)
–snip–
The root of such incorrect comparisons may be a knowledge gap regarding how seasonal influenza and COVID-19 data are publicly reported. The CDC, like many similar disease control agencies around the world, presents seasonal influenza morbidity and mortality not as raw counts but as calculated estimates based on submitted International Classification of Diseases codes.2 Between 2013-2014 and 2018-2019, the reported yearly estimated influenza deaths ranged from 23 000 to 61 000.3 Over that same time period, however, the number of counted influenza deaths was between 3448 and 15 620 yearly.4 On average, the CDC estimates of deaths attributed to influenza were nearly 6 times greater than its reported counted numbers. Conversely, COVID-19 fatalities are at present being counted and reported directly, not estimated. As a result, the more valid comparison would be to compare weekly counts of COVID-19 deaths to weekly counts of seasonal influenza deaths.
During the week ending April 21, 2020, 15 455 COVID-19 counted deaths were reported in the US.5 The reported number of counted deaths from the previous week, ending April 14, was 14 478. By contrast, according to the CDC, counted deaths during the peak week of the influenza seasons from 2013-2014 to 2019-2020 ranged from 351 (2015-2016, week 11 of 2016) to 1626 (2017-2018, week 3 of 2018).6 The mean number of counted deaths during the peak week of influenza seasons from 2013-2020 was 752.4 (95% CI, 558.8-946.1).7 These statistics on counted deaths suggest that the number of COVID-19 deaths for the week ending April 21 was 9.5-fold to 44.1-fold greater than the peak week of counted influenza deaths during the past 7 influenza seasons in the US, with a 20.5-fold mean increase (95% CI, 16.3-27.7).5,6
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2766121?
Yah. Just like the flu.
Discussion here of challenge trials…
https://www.npr.org/transcripts/847755751
As well as coronavirus antibody dependent enhancement
> Since the 1960s, tests of vaccine candidates for diseases such as dengue, respiratory syncytial virus (RSV), and severe acute respiratory syndrome (SARS) have shown a paradoxical phenomenon: Some animals or people who received the vaccine and were later exposed to the virus developed more severe disease than those who had not been vaccinated (1). The vaccine-primed immune system, in certain cases, seemed to launch a shoddy response to the natural infection. “That is something we want to avoid,” says Kanta Subbarao, director of the World Health Organization Collaborating Centre for Reference and Research on Influenza in Melbourne, Australia.
https://www.pnas.org/content/117/15/8218
Joshua
“The root of such incorrect comparisons may be a knowledge gap regarding how seasonal influenza and COVID-19 data are publicly reported.”
DK Young has no knowledge gaps. He’s made sure we know that.
I believe they have done some work on ADE in Toronto where they have people who became ill after contact with SARS-CoV-1. I don’t think they’re seeing it. Fauci mentioned it the other day while discussing problems that could arise with a rushed virus, which is why we need to elect infectious disease doctors.
JCH –
Yah. ADE as a concern during vaccine development…
BBC News mentioned this morning that there has been a monkey trial where “challenged” monkeys didn’t get a fever and didn’t get an exaggerated, harmful immune response. I presume this is it:
https://uk.reuters.com/article/us-health-coronavirus-vaccine-oxford/oxford-coronavirus-vaccine-found-protective-in-small-monkey-study-idUKKBN22Q32G
So presumably it keeps them safe, but unfortunately they can still infect others.
Can’t find the preprint but haven’t searched very hard.
Oh, and Estimating the burden of SARS-CoV-2 in France.
A Spanish study also published on Wednesday showed similar results, saying about 5% of the country’s population had contracted the disease and that there was no herd immunity in Spain, also emerging progressively for long lockdown.
The UK ONS pilot infection survey came back with an infection rate of 0.27%, “at any given time between 27 April and 10 May 2020”. IOW they returned swabs taken on that date from about a month after lockdown, which tested positive. It excludes people in care homes and hospitals, so is a biased sample (by design, to assess community infection). I suppose for completeness you should add those admitted to hospital and tested positive during that period (about 60,000 according to worldometer) to their estimate of 148,000 (94,000 – 222,000) infected in England. Minus any of the volunteers who were admitted to hospital after returning their swab, and minus the relatively small about 15% by population proportion of UK hospital cases outside England.
I think a certain dead parrot that had been nailed to its perch by a handful of contrarians has now fallen off its perch.
OK. This is the man, who many “skeptics” and a really large # of Americans, think has the right approach with this pandemic.
> In a speech on Thursday at Owens and Minor, a medical supply distributor located in Allentown, PA, President Donald Trump wondered whether testing for Covid-19 coronavirus is “overrated.” He then proceeded to say, “And don’t forget, we have more cases than anybody in the world. But why? Because we do more testing.”
Next, he clarified: “When you test, you have a case. When you test, you find something is wrong with people. If we didn’t do any testing, we would have very few cases.”
***************
I suppose that might be true, in a very generous reading, if a really large % of those tested were asymptomatic. But that isn’t the case.
But regardless, I’m increasingly thinking that if magical thinking doesn’t warp spacetime, and the virus doesn’t just goes away, or we don’t hit herd immunity at a really low % of the population, or we don’t get a vaccine incredibly fast, or we just don’t decide that we don’t care about a lot of old people dying and younger people getting sick, and we just don’t stop caring about healthcare workers and disparities in deaths association with race/ethnicity/wealth, in the US we are totally fucked.
it seems stupidity is the real pandemic
So –
My “friend” thought his/her questions about climate modeling weren’t answered. Now I know it’s kind of weird that I’m posting his/her questions instead of him/her doing so…but for some reason I don’t quite understand my friend didn’t want to post here him/herself and I’m kind of curious about this issue to the extent I can understand any of it.
And I thought posting his/her question last time prompted an interesting discussion. So with those caveats, he/she wrote…
–snip–
But I want to emphasize there is nothing theoretical or philosophical about it… The response I am looking for is “here is how it is actually calculated, you got confused” and some code or equations are shown yielding the correct range that do not depend the amount of scatter around the forcing vs deltaT line (which is a descriptive property of the data, and will not change unless the underlying process that generates the data changes).
I don’t think anyone in that discussion has ever looked into how that range is actually arrived it.
The 1.5-4.5 C range is due to variability instead of uncertainty *by definition*. It is like a standard deviation, not a confidence interval.
There is nothing theoretical or philosophical about it… The response I am looking for is “here is how it is actually calculated, you got confused” and some code or equations are shown yielding the correct range that do not depend the amount of scatter around the forcing vs deltaT line (which is a descriptive property of the data, and will not change unless the underlying process that generates the data changes).
–snip–
Now in response to that, I said: “I’m confused because it seemed to me there was general agreement (albeit more for some than others) that the range of the estimate may well be a property of the data, and might not change. What am I missing?”
Which netted a response that:
–snip–
You’ll have to quote where you saw that. I saw the exact opposite. Discussion of hypothetical earths, aleatory uncertainty, thinking the range will get smaller as more data is collected, etc.
I’d also say link the original post, which I admit is hard to follow without equations (which can be seen in the paper I cute though) and a graph: https://statmodeling.stat.columbia.edu/2015/12/10/28302/#comment-254706
–snip–
So here’s the “original post”
https://statmodeling.stat.columbia.edu/2015/12/10/28302/#comment-254706
“But I want to emphasize there is nothing theoretical or philosophical about it… ”
err, no, defining what type of uncertainty you are talking about is central to the question.
If you mean the IPCC interval, there is no code that calculates it, IIRC, it is a statement of expert consensus opinion.
“You’ll have to quote where you saw that. I saw the exact opposite. Discussion of hypothetical earths, aleatory uncertainty, thinking the range will get smaller as more data is collected, ”
I think it would be more correct to say that the range will get smaller as our understanding improves (which will be partly due to the collection of data, but only partly – you have to extract knowledge from the data first).
an_older_code sez …
“it seems stupidity is the real pandemic”
Beat you on that one …
“In the US we have had a different virus. for several decades now, it is called stupidity. It is exacerbated by a dipshit POTUS, aka Small Hands, and COVID-19.”
“it seems stupidity is the real pandemic”
it’s only been going for 300,000 years or so, perhaps there will be a vaccine at some point?
“perhaps there will be a vaccine at some point?”
I’m going to go with a brain-machine neuro-interface which will rewrite our memories.
First they will let us control machines via our thoughts:
Next they will reverse the process and rewrite/create memories and that will eradicate ‘stupidity’.
Maybe like “lucid dreaming” but the dream is implanted:
https://www.syfy.com/syfywire/new-mit-device-dormio-hacks-dreams
Joshua – The comment you linked led to a Science article which ended with the following quote:
“We are constrained by the inevitable: the more likely a large warming is for a given forcing (i.e., the greater the positive feedbacks), the greater the uncertainty will be in the magnitude of that warming.”
Implies a bit of a catch-22, the more certain we become about strong sensitivity, the harder it is to pin down.
Quarantine process at inchon airport is a paperwork nightmare. Plane was packed with bunny suit wearing people. I’m sitting with about 20 people under police guard. Waiting for our special bus
@ EFS and DM
well that’s the irony we have done so much in the last 120 years to unlock the secrets of the universe
yet we have to wonder about he efficacy of injecting bleach
Willard – I was way ahead of that guy.
@ SM
https://www.theguardian.com/world/2020/may/15/flying-long-haul-during-covid-19-air-travel-has-never-been-stranger
Speaking of flying, some news from JetBlue:
https://www.buzzfeednews.com/article/stephaniemlee/stanford-coronavirus-neeleman-ioannidis-whistleblower
Imagine what David Young would say if climate modellers ever did that.
Willard –
My jaw kept dropping closer and closer to the floor as I read that further into that article.
So good that we have folks like John around to champion for scientific integrity in research.
> Others had received an email from Bhattacharya’s wife, falsely claiming that an “FDA approved” test would definitively reveal if they could “return to work without fear,” as BuzzFeed News has reported.
What an embarrassment. Not only should Bendavid get fired, so should the entire IRB at Stanford.
Assuming what’s in the article is true.
Wikkard (and JCH),
Thanks for those two very informative articles (e. g. travel closures and Stanford exposés).
Willard not Wikkard.
Willard –
Seen this?:
https://oklahoman.com/article/5660312/coronavirus-in-oklahoma-oklahoman-behind-population-testing-for-covid-19-antibodies/amp?__twitter_impression=true
I came up with the 12-airport theory the night I saw it on the news. Any rancher making a decision like that ends up with a whole bunch of dead cattle. It was stupid as it gets.
Those who oppose an honest, skeptical observation of reality use semantics to distract, deny, and delay. There is no combination of words that will overcome this, they’ll just shift until they find a new way to undermine the truth. I find even writing this, and I love words, I cannot say a single thing without trying to find a clearer, better, unexceptionable way to say what is, is, and failing. Giving in to redefining terms is not going to “win”. Words are an imperfect approximation: semantics used as weapon and defense create an equality that is not there in the facts. It might be better to ignore this high-class trolling and present what is real from it’s core, rather than as a response to the legion of arguments that grow like dragon’s teeth in that hoary old Greek story.
Striving for perfection is very nice, but getting on with it as best we can is better, imnsho.
Meanwhile – for our friends in the UK
https://twitter.com/CT_Bergstrom/status/1261058066495074304?s=20
I wouldn’t want you all to feel left out.
Joshua,
Yes, I saw that. Pretty deadful paper.
Makes the Santa Clara study look Nobel-worthy in comparison.
Quick refresher course for NBC News in the three-beat, “truth sandwich” method.
1) State what is true.
2) Report that a false claim has been made. (But only if it’s newsworthy, meaning important for the public to know it happened.)
3) Repeat what the truth actually is.
Susan,
Just came across the news that your father had died. My condolences.
ATTP:
“As Eli points out, science often (mostly) does involve being aware of a consensus. Scientists don’t reinvent the wheel everytime they do some research; they’re often working within some framework that is currently supported by the evidence. This is what I would regard as a consensus position. Of course, some scientists might be trying to challenge this, but even doing so requires an understanding of what it is”
Echo chamber dwellers who don’t understand the climate models they reject may put thmselves at risk by rejecting epedemiological modeling and modern medicine just they disparage the climate consensus”
The rise of viral denial among the WUWT and Climate Etc commentariat has gotten scary enough to make even Christopher Monckton balk:
https://vvattsupwiththat.blogspot.com/2020/05/primum-non-nocere.html
Willard
“Imagine what David Young would say if climate modellers ever did that.”
I think it would depend on what the climate model’s results were, right?
Confirming that a Corona Test is not fun.
Long Version.
I always seem to occupy ( probably by choice) a grey zone.
So at the airport they did not know what to do with me.
Rules are short stay Visa in Korea ( 90 day) must all report to Hotel quarantine.
However, in the early questioning they did determine that I had a residence in Seoul
( cause I brought my lease) And so initially I was slated to go home. and so I was registered
with the tracking app. This works to report your conditions and to real time GPS track you
so you dont leave ur house. Phone is tested.. I am good to go home.
During this process supervisors were called half a dozen times to see how to handle me.
They assume all short stay people have no residence. And here was the exceptional mosher.
Any way, after filling out a bazillion forms and agreements I was getting ready to exit.
and they caught me at the last check point. It was off to a different office for more
interviewing ext. And they called my roommate in Korea, and there was another exception.
Not blood related, therefore I must go to government Quarantine.
In reality I had planned for this all along but was hoping to avoid it since the rules had an apparent loophole.
next up was waiting to be transported by bus to a Seoul Hotel. probably a 2 hour wait guarded by police, I found the smoking cop and we hit the smoking room together.
I should probably write something up as I took pictures at every step.
I have paid my bill ~1200 USD for the 14 nights and 15 days I will spend here.
https://www.hotel-marinabay.co.kr/
They snuck us in through the back door, So I am not sure if they have other guests or not.
Before you think it is a luxury place, my room is two single beds. Here are the rulz
1. No smoking, no leaving your room.
2. no deliveries or visitors.
3. meals served 3x daily. They announce delivery you open the door grab your food.
4. Put your trash out 1 time a day in orange bio hazard bags.
5. Given the food delivered I project a 10lb weigh loss
This morning I got nose probed and throat probed.
Yikes, pretty deep on both
Odd, it was really enjoyable to read that.
Welcome JCH. Before I thought I would go back to China and do a Quarantine there so I was happy to read some foreigners description of the process. Pretty similar.
Except in China you were given a choice of 14 hotels around Beijing.
Compared to the US procedure of just letting people come in, I do find this approach and the
China approach more sensible and in the end more humane.
I had to laugh on my trip to the US. They passed out a silly card from the CDC. “please stay in your home for 14 days” stupid fuckers, I got off the plane, went to a hotel and got back to Korea.
It is kinda weird waiting around all day for the intercom messages : your meal will be placed
outside your door. Please pick it up quickly, wash your hands with soap and water for 30 seconds
and dry them.
aTTP: I’m inclined to celebrate Philip Anderson’s life rather than mourn his passing. He was 96 and ready to go. They think there’s been a breakthrough on his “spin” theories (forgive layperson imprecision), and it’s too bad he won’t get to see that if it pans out. Oxford University Press plans to bring out his biography in December. If anybody who understands physics properly wants to figure out what I’m trying to say about spin, here’s Phuan Ong’s latest: https://scholar.google.com/scholar?as_ylo=2020&q=phuan+ong+spin&hl=en&as_sdt=0,22&as_vis=1
Susan,
Certainly a life full of impressive achievements.
This is interesting, and it is a pity that he won’t get to see if it pans out.
I don’t often read biographies, but I’ll endeavour to read this one.
CDC finds* a 0.28% crude mortality rate to date in NYC. There is reason to believe it could triple before herd immunity is reached meaning it could reach 1% before this is through. If so, there is no chance that IFR is < 0.28%, and possibly much higher than 1%.
*CDC estimated actual COVID-19 deaths in NYC by analyzing the "excess deaths". CMR is derived directly from that.
It’s easier to assess claims after evidence accumulates on them. So now that months have passed, we can assess some of the false claims dpy6629 made:
Re:
“The best serologic study was probably in Miami Dade county where they did a random sample. Taking the fatality number for 21 days after the median testing date, the IFR is 0.17% to 0.31%. This is likely an overestimation as most people use a 14 day delay.”
Miami-Dade later decreased their seroprevalence estimate from 6% (thereby increasing any IFR estimated from it), possibly due to issues with their original testing protocol:
old: https://miamidade.gov/releases/2020-04-24-sample-testing-results.asp
new: https://web.archive.org/web/20200727041934/http://www.sparkc.info/
Re:
“But this is mostly irrelevant because there are now 3 studies that give much the same conclusions. Santa Clara, Los Angeles, and Miami Dade.
The Santa Clara suffered from a number of crucial flaws, including a recruitment design that would over-estimate seroprevalence, reportedly misleading statements used to recruit subjects, inadequate corrections for sensitivity/specificity, funding issues, etc.:
https://academic.oup.com/jid/article/doi/10.1093/infdis/jiaa429/5872489
https://www.medrxiv.org/content/10.1101/2020.04.24.20078824v1
https://www.medrxiv.org/content/10.1101/2020.05.03.20089201v1
https://tandfonline.com/doi/full/10.1080/13669877.2020.1778771
https://www.nature.com/articles/d41586-020-01095-0
https://science.sciencemag.org/content/368/6489/350.full
https://buzzfeednews.com/article/stephaniemlee/stanford-coronavirus-neeleman-ioannidis-whistleblower
https://buzzfeednews.com/article/stephaniemlee/stanford-coronavirus-study-bhattacharya-email
So it’s very unlikely to be representative of the general population in Santa Clara. Fortunately, there’s a better study underway in Santa Clara:
http://med.stanford.edu/epidemiology-dept/research/covid-research-collaborative/CA-Facts.html
The Los Angeles County study was followed by a large increase in COVID-19 deaths, making deaths hard to pair with corresponding infections and thus reducing the reliability of IFR inferred from it:
https://www.medrxiv.org/content/10.1101/2020.07.23.20160895v3
Re:
“Thanks Steven, For Arizona, taking the death number from 14 days after the mean test date is what Ioannidis et al did.”
There’s no evidence I know of that the Arizona results were from a randomized sample representative of the general population in Arizona:
Re:
“My main point is just that as evidence is accumulating, the best evidence seems to show IFR’s between 0.12% and 0.4%.”
We now have studies from different parts of the US showing an IFR of 0.5% or more. And if we look more globally at seroprevalence-based IFR estimates, the studies with the least risk of bias show an IFR of ~0.5% – ~1.5%:
https://www.medrxiv.org/content/10.1101/2020.07.23.20160895v3
Some other examples of seroprevalence-based IFR estimates from the USA:
1.6% : https://wwwnc.cdc.gov/eid/article/26/11/20-3029_article
1.3% : https://louisville.edu/medicine/news/phase-ii-results-of-co-immunity-project-show-higher-than-expected-rates-of-exposure-to-novel-coronavirus-in-jefferson-county
0.8% (higher if one accounts for right-censoring) : https://washoecounty.us/outreach/2020/07/2020-07-08-jic-update-0708.php
0.6% : https://sciencedirect.com/science/article/pii/S1047279720302015
0.6% : https://cdc.gov/mmwr/volumes/69/wr/mm6929e1.htm
consistent with 0.5% – 1.0% : http://archive.is/JXtUt#selection-1159.0-1163.200 [ https://rivcoph.org/Portals/0/Documents/CoronaVirus/July/News/7.27.20%20antibody%20testing%20results.pdf?ver=2020-07-27-144931-703×tamp=1595886602504 ]
Hence why the CDC upgraded their best estimate of IFR to 0.65%, even though that’s also likely an under-estimate, as acknowledged by a soon-to-be-updated draft of the study they cite for that estimate:
table 1 of: https://web.archive.org/web/20200823001414/https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html
“Restricting the analysis to only those studies at a low risk of bias resulted in modestly reduced heterogeneity and an increased IFR of 0.76% (0.37-1.15%). […] It is not unlikely that, after correcting for excess mortality not captured in official death reporting systems, the IFR of COVID-19 in most populations would be higher than 1%.”
Click to access 2020.05.03.20089854v4.full.pdf
Update:
Re:
“This is 3-5 times lower than Ferguson’s initial estimates. That’s a very big difference.”
Ferguson et al.’s IFR was ~0.9% for Great Britain:
Click to access 2020-03-16-COVID19-Report-9.pdf
That did not over-estimate observed seroprevalence-based IFR, including if one takes age-stratification into account:
https://www.medrxiv.org/content/10.1101/2020.07.23.20160895v3
https://www.medrxiv.org/content/10.1101/2020.08.12.20173690v2 [see supplementary table S2(a)]
https://doi.org/10.1016/S2468-2667(20)30135-3
https://www.medrxiv.org/content/10.1101/2020.05.03.20089854v4
Re:
“I’m more thinking of his Diamond Princess study (I think in early March as well) which has very similar numbers to the Santa Clara study.”
No, the Diamond Princess results are not similar to the Santa Clara result. Applying the Diamond Princess data to a country ends up with an IFR in the range of ~0.5% or more, which is larger than dpy6629 claims. 14 people died of COVID-19 for the Diamond Princess (13 under Japan’s purview, and one reported for Australia):
https://science.sciencemag.org/content/368/6498/eabd4246.full [ https://en.wikipedia.org/wiki/COVID-19_pandemic_on_Diamond_Princess ; https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30364-9/fulltext ]
https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30243-7/fulltext
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7118348/
Re:
“Further, as has been known from the beginning, this virus is vastly more serious for those over 65 or those who are already seriously ill.”
The virus is a serious risk even to middle-aged people and even in comparison to the risk of mortality from other events, such as automobile accidents:
https://www.medrxiv.org/content/10.1101/2020.07.23.20160895v3
Re:
“The simple fact of the matter is that governments have made decisions based on extremely uncertain science whose estimates have proved to be quite wrong.”
That was followed up by a reference to John Ioannidis, who, ironically, does not agree with dpy6629 on this point, especially as applied to climate science:
“Many fields lack the high reproducibility standards that are already used in fields such as air pollution and climate change. […] It is a scandal that the response of governments to climate change and pollution has not been more decisive.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5933781/
Re:
“I see that Schmidt, someone with no knowledge of epidemiology, attacks an expert with a very strong track record.”
dpy6629 should be careful about making this point on expertise, since his critics often have more expertise in this subject than he does.
“As an immunologist, I can say what you just wrote makes no sense and has been repeatedly debunked in the scientific literature.”
Atomsk –
Thanks for the links. David will NEVER accept any of this, of course, He will simply repeat that Ioannidis is correct no matter what the evidence is
As for this:
> The Santa Clara suffered from a number of crucial flaws,
For me, the more critical issue there is the ethically dubious aspect of how the study was conducted – specifically promising participants an “immunity passport” if they tested positive without telling people that they could be getting a false positive test and necessarily should repeat the testing before assuming that they couldn’t be infectious and going to visit grandma.
It will be interesting to see what happens with the whistleblower complaint.
I also can’t believe that they either got IRB approval for recruiting through an email sent out be a researchers spouse, or used that recruitment method without telling the IRB. It’s really bad methodology and either really sloppy or again unethical research practice. The whole set of behaviors on the part of those researchers – with their public policy advocacy, is really a mess.
Re:
“For me, the more critical issue there is the ethically dubious aspect of how the study was conducted […]”
Fair enough, though in principle, even ethically dubious research can lead to accurate results. Of course that doesn’t imply in this case because their misleading recruitment pitch would likely skew their population, such as in favor of people more eager to return to employment. And like you, I’m curious about how the whistleblower complaint turns out.
Re:
“Thanks for the links. David will NEVER accept any of this, of course, He will simply repeat that Ioannidis is correct no matter what the evidence is”
…except when Ioannidis discusses the reproducibility of climate science results and how those results should impact government policy:
“Ioannidis can be wrong on some issues even though generally his statistical work seems sound to me.”
Anyway, I should probably say something on Ioannidis then, since David keeps elevating him. So many others covered Ioannidis’ COVID-19 distortions. For example:
https://www.medscape.com/viewarticle/931538
https://twitter.com/AVG_Joseph96/status/1262820843802984449
https://hildabastian.net/index.php/91
https://academic.oup.com/jid/advance-article/doi/10.1093/infdis/jiaa429/5872489
But to touch on a few points:
1) Ioannidis predicted less than 40,000 USA COVID-19 deaths. We’re at about 177,000 now and still increasing [that 177,000 is an under-estimate, if one looks at excess deaths]:
http://archive.is/dT97F#selection-2211.202-2219.279
2) Ioannidis projected ~10,000 USA COVID-19 deaths using his Diamond-Princess-derived CFR of ~0.3%, despite the fact that even at that time his CFR was known to be multiple factors too low [I went over Diamond-Princess-derived fatality rates in my previous comment]:
https://www.statnews.com/2020/03/17/a-fiasco-in-the-making-as-the-coronavirus-pandemic-takes-hold-we-are-making-decisions-without-reliable-data/
3) His work on IFR has been repeatedly criticized for using non-representative samples that conveniently skew IFR lower, being non-systematic, etc. If folks want a good catalog of the problems with the types of studies Ioannidis often uses, then they should see the methodology section of:
https://www.medrxiv.org/content/10.1101/2020.07.23.20160895v3
Ioannidis seemingly uses motivated reasoning to reach his pre-determined conclusion of a low IFR and lower risk from COVID-19, even when his claims conflict with the evidence. One of the clearest examples of this was when he claimed a Brazilian study showed an IFR of ~0.3%, when the study actually showed an IFR of ~1%. Ioannidis’ rationale for his claim conflicted with how he inferred IFR from other studies and his rationale was unsound (ex: his method fails to take into account how Brazilian regions with a larger population size would play a relatively larger role in determining Brazil’s average IFR):
I don’t know how any informed, somewhat less-biased person could keep claiming Ioannidis was correct. He’s done great damage to his reputation, seemingly in service of the political ideology he shares with at least one of his Santa Clara study co-authors at Stanford:
“An Elite Group Of Scientists Tried To Warn Trump Against Lockdowns In March
[…]
John Ioannidis’s controversial studies claim that the coronavirus isn’t that big a threat. Before the Stanford scientist did any of them, he wanted to take that message to the White House.”
https://www.buzzfeednews.com/article/stephaniemlee/ioannidis-trump-white-house-coronavirus-lockdowns
https://www.hoover.org/profiles/jay-bhattacharya
Good to have Atomsk’s Sanakan updates. I do recall from earlier that A.S.has credentials or qualifications in epidemiology, and that this David P. Young is really a piece of work.
Just to clarify: as I mentioned above, I’m an immunologist, not an epidemiologist.
I know a bit of epidemiology, since some of that is needed for understanding immunology, infections, etc. But I don’t have the level of expertise as some of Ioannidis’ critics, like the epidemiologist GidMK (Gideon Meyerowitz-Katz). So I often run what I say by Meyerowitz-Katz on Twitter, and he seems interested enough. In any event, you don’t need to know much about epidemiology to see where Ioannidis and David messed up. The immunology comes more in handy when addressing the distortions Nic Lewis and others offer on herd immunity, cross-reactive T cells, individual susceptibility to infection, the origins of SARS-CoV-2 (ex: what its immunoevasion says about its origins), etc. I’ve corrected those distortions often enough that Judith Curry is now just blocking my comments.
“The dangerous myth that Sweden achieved herd immunity”
View at Medium.com
> …except when Ioannidis discusses the reproducibility of climate science results and how those results should impact government policy:
It’s his advocacy that is most troublesome for me. Estimates can be wrong (he somewhat caveated his 40,000 prediction). But to go on national TV to mischaracterizes the IC projection and then call it “science fiction,” to treat uncertainty selective (e. g., taking about “died with” vs. “died from” but not talking about people who died at home without testing), to say that covid is no more dangerous than the seasonal flu, to not differentiate between economic impact from “lockdowns” and impact from the pandemic itself etc…etc…